

Progress report on the first sub-Saharan Africa trial of newer versus older antihypertensive drugs in native black patients
- PMID: 22594907
- PMCID: PMC3502563
- DOI: 10.1186/1745-6215-13-59
Progress report on the first sub-Saharan Africa trial of newer versus older antihypertensive drugs in native black patients
Abstract
Background: The epidemic surge in hypertension in sub-Saharan Africa is not matched by clinical trials of antihypertensive agents in Black patients recruited in this area of the world. We mounted the Newer versus Older Antihypertensive agents in African Hypertensive patients (NOAAH) trial to compare, in native African patients, a single-pill combination of newer drugs, not involving a diuretic, with a combination of older drugs including a diuretic.
Methods: Patients aged 30 to 69 years with uncomplicated hypertension (140 to 179/90 to 109 mmHg) and ≤2 associated risk factors are eligible. After a four week run-in period off treatment, 180 patients have to be randomized to once daily bisoprolol/hydrochlorothiazide 5/6.25 mg (R) or amlodipine/valsartan 5/160 mg (E). To attain blood pressure <140/<90 mmHg during six months, the doses of bisoprolol and amlodipine should be increased to 10 mg/day with the possible addition of up to 2 g/day α-methyldopa.
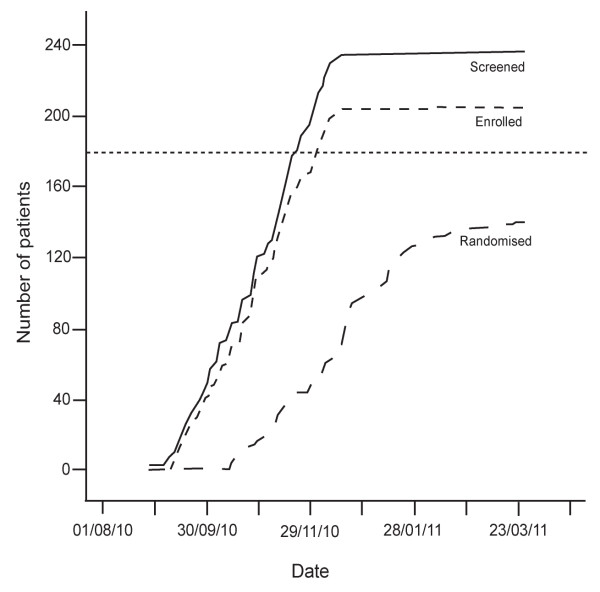
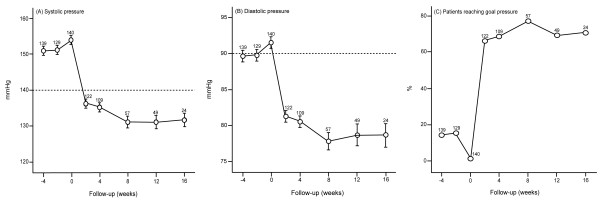
Results: At the time of writing of this progress report, of 206 patients enrolled in the run-in period, 140 had been randomized. At randomization, the R and E groups were similar (P ≥ 0.11) with respect to mean age (50.7 years), body mass index (28.2 kg/m(2)), blood pressure (153.9/91.5 mmHg) and the proportions of women (53.6%) and treatment naïve patients (72.7%). After randomization, in the R and E groups combined, blood pressure dropped by 18.2/10.1 mmHg, 19.4/11.2 mmHg, 22.4/12.2 mmHg and 25.8/15.2 mmHg at weeks two (n = 122), four (n = 109), eight (n = 57), and 12 (n = 49), respectively. The control rate was >65% already at two weeks. At 12 weeks, 12 patients (24.5%) had progressed to the higher dose of R or E and/or had α-methyldopa added. Cohort analyses of 49 patients up to 12 weeks were confirmatory. Only two patients dropped out of the study.
Conclusions: NOAAH (NCT01030458) demonstrated that blood pressure control can be achieved fast in Black patients born and living in Africa with a simple regimen consisting of a single-pill combination of two antihypertensive agents. NOAAH proves that randomized clinical trials of cardiovascular drugs in the indigenous populations of sub-Saharan Africa are feasible.
Figures


Similar articles
-
Rationale and design of the Newer Versus Older Antihypertensive Agents in African Hypertensive Patients (NOAAH) trial.Blood Press. 2011 Oct;20(5):256-66. doi: 10.3109/08037051.2011.572614. Epub 2011 Apr 15. Blood Press. 2011. PMID: 21495829 Clinical Trial.
-
Efficacy of newer versus older antihypertensive drugs in black patients living in sub-Saharan Africa.J Hum Hypertens. 2013 Dec;27(12):729-35. doi: 10.1038/jhh.2013.56. Epub 2013 Jun 27. J Hum Hypertens. 2013. PMID: 23803591 Free PMC article. Clinical Trial.
-
Real-world effectiveness of amlodipine/valsartan and amlodipine/valsartan/hydrochlorothiazide in high-risk patients and other subgroups.Vasc Health Risk Manag. 2015 Jan 21;11:71-8. doi: 10.2147/VHRM.S76599. eCollection 2015. Vasc Health Risk Manag. 2015. PMID: 25653536 Free PMC article.
-
Valsartan-amlodipine-hydrochlorothiazide: the definitive fixed combination?Expert Rev Cardiovasc Ther. 2010 Nov;8(11):1609-18. doi: 10.1586/erc.10.115. Expert Rev Cardiovasc Ther. 2010. PMID: 21090936 Review.
-
Amlodipine and valsartan as components of a rational and effective fixed-dose combination.Vasc Health Risk Manag. 2009;5(1):165-74. doi: 10.2147/vhrm.s3134. Epub 2009 Apr 8. Vasc Health Risk Manag. 2009. PMID: 19436661 Free PMC article. Review.
Cited by
-
The coArtHA trial-identifying the most effective treatment strategies to control arterial hypertension in sub-Saharan Africa: study protocol for a randomized controlled trial.Trials. 2021 Jan 21;22(1):77. doi: 10.1186/s13063-021-05023-z. Trials. 2021. PMID: 33478567 Free PMC article.
-
Nigerian Population Research on Environment, Gene and Health (NIPREGH) - objectives and protocol.J Biomed Res. 2014 Sep;28(5):360-7. doi: 10.7555/JBR.28.20130199. Epub 2014 Jun 19. J Biomed Res. 2014. PMID: 25332707 Free PMC article.
-
Difference in blood pressure response to ACE-Inhibitor monotherapy between black and white adults with arterial hypertension: a meta-analysis of 13 clinical trials.BMC Nephrol. 2013 Sep 26;14:201. doi: 10.1186/1471-2369-14-201. BMC Nephrol. 2013. PMID: 24067062 Free PMC article.
-
Formulations of Amlodipine: A Review.J Pharm (Cairo). 2016;2016:8961621. doi: 10.1155/2016/8961621. Epub 2016 Oct 16. J Pharm (Cairo). 2016. PMID: 27822402 Free PMC article. Review.
-
A review of the efficacy and tolerability of combination amlodipine/valsartan in non-white patients with hypertension.Am J Cardiovasc Drugs. 2013 Oct;13(5):301-13. doi: 10.1007/s40256-013-0033-4. Am J Cardiovasc Drugs. 2013. PMID: 23784267 Free PMC article. Review.
References
-
- Bonita R, Reddy S, Galbraith S, Bettcher D, MacIntyre M, Peden M, Rozenberg M, Vu C. In: The World Health Report 2003 - Shaping the Future. Beaglehole R, Irwin A, Prentice T, editor. World Health Organization, Geneva, Switzerland; 2003. Neglected global epidemics: three growing threats; pp. 83–102.
-
- Donnison C. Blood pressure in African natives: its bearing on the aetiology of hyperpiesa and arteriosclerosis. Lancet. 1929;i:6–7.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
