

Prevalence of Kawasaki disease in young adults with suspected myocardial ischemia
- PMID: 22595319
- PMCID: PMC3393523
- DOI: 10.1161/CIRCULATIONAHA.111.082107
Prevalence of Kawasaki disease in young adults with suspected myocardial ischemia
Abstract
Background: Up to 25% of patients with untreated Kawasaki disease (KD) and 5% of those treated with intravenous immunoglobulin will develop coronary artery aneurysms. Persistent aneurysms may remain silent until later in life when myocardial ischemia can occur. We sought to determine the prevalence of coronary artery aneurysms suggesting a history of KD among young adults undergoing coronary angiography for evaluation of possible myocardial ischemia.
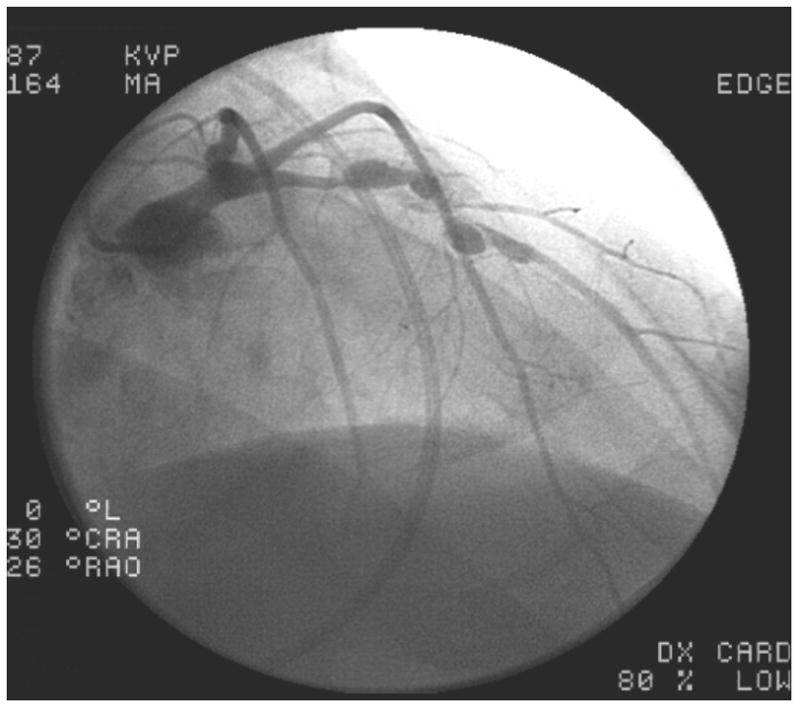
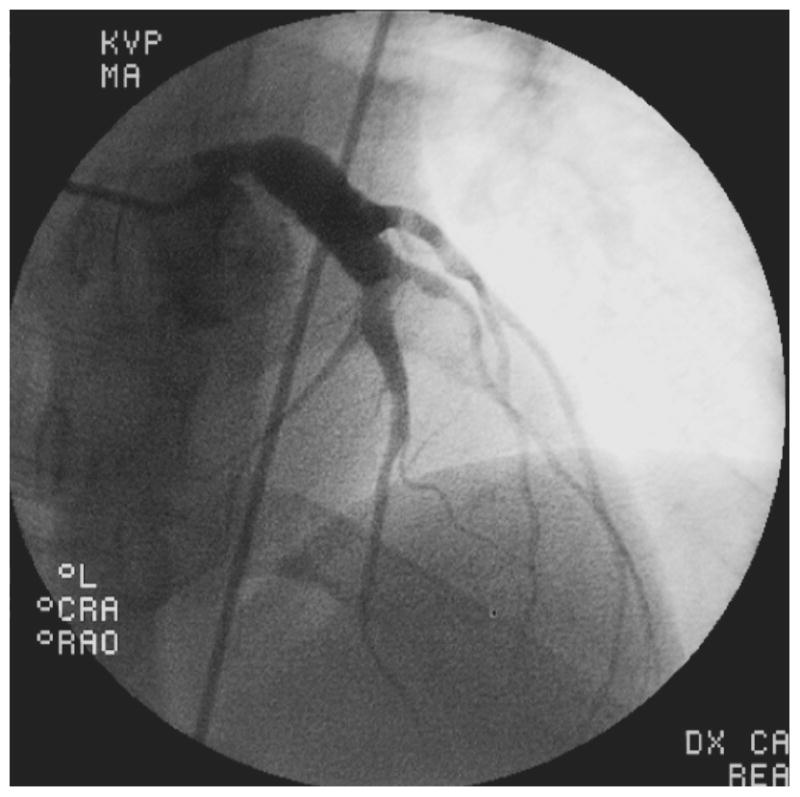
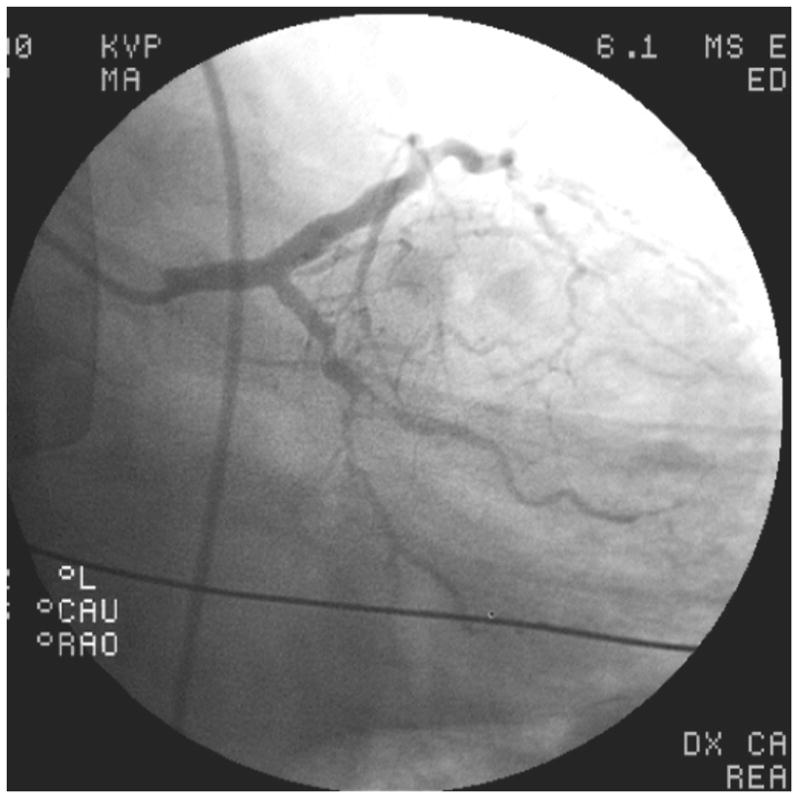
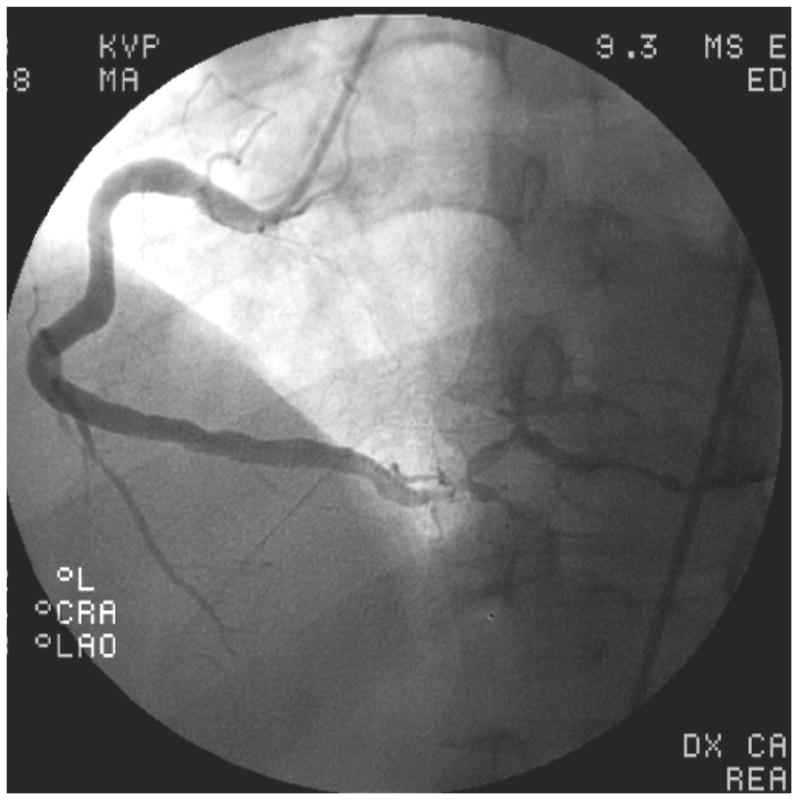
Methods and results: We reviewed the medical histories and coronary angiograms of all adults <40 years of age who underwent coronary angiography for evaluation of suspected myocardial ischemia at 4 San Diego hospitals from 2005 to 2009 (n=261). History of KD-compatible illness and cardiac risk factors were obtained by medical record review. Angiograms were independently reviewed for the presence, size, and location of aneurysms and coronary artery disease by 2 cardiologists blinded to the history. Patients were evaluated for number of risk factors, angiographic appearance of their coronary arteries, and known history of KD. Of the 261 young adults who underwent angiography, 16 had coronary aneurysms. After all clinical criteria were assessed, 5.0% had aneurysms definitely (n=4) or presumed (n=9) secondary to KD as the cause of their coronary disease.
Conclusions: Coronary sequelae of KD are present in 5% of young adults evaluated by angiography for myocardial ischemia. Cardiologists should be aware of this special subset of patients who may benefit from medical and invasive management strategies that differ from the strategies used to treat atherosclerotic coronary artery disease.
Conflict of interest statement
Figures



Comment in
-
Coronary artery disease: Consider Kawasaki disease when assessing myocardial ischemia.Nat Rev Cardiol. 2012 Jun 5;9(7):375. doi: 10.1038/nrcardio.2012.82. Nat Rev Cardiol. 2012. PMID: 22665324 No abstract available.
References
-
- Newburger JW, Takahashi M, Beiser AS, Burns JC, Bastian J, Chung KJ, Colan SD, Duffy CE, Fulton DR, Glode MP, Mason WH, Cody Meissner H, Rowley AH, Shulman ST, Reddy V, Sundel RP, Wiggings JW, Colton T, Melish ME, Rosen FS. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med. 1991;324:1633–1639. - PubMed
-
- Kato H, Inoue O, Kawasaki T, Fujiwara H, Watanabe T, Toshima H. Adult coronary artery disease probably due to childhood Kawasaki disease. Lancet. 1992;340:1127–1129. - PubMed
-
- Burns JC, Shike H, Gordon JB, Malhotra A, Schoenwetter M, Kawasaki T. Sequelae of Kawasaki disease in adolescents and young adults. J Am Coll Cardiol. 1996;28:253–257. - PubMed
-
- Kato H, Sugimura T, Akagi T, Sato N, Hashino K, Maeno Y, Kazue T, Eto G, Yamakawa R. Long-term consequences of Kawasaki disease. A 10- to 21-year follow-up study of 594 patients. Circulation. 1996;94:1379–1385. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
