

Temporal trends in and factors associated with bleeding complications among patients undergoing percutaneous coronary intervention: a report from the National Cardiovascular Data CathPCI Registry
- PMID: 22595404
- PMCID: PMC3908898
- DOI: 10.1016/j.jacc.2011.12.045
Temporal trends in and factors associated with bleeding complications among patients undergoing percutaneous coronary intervention: a report from the National Cardiovascular Data CathPCI Registry
Abstract
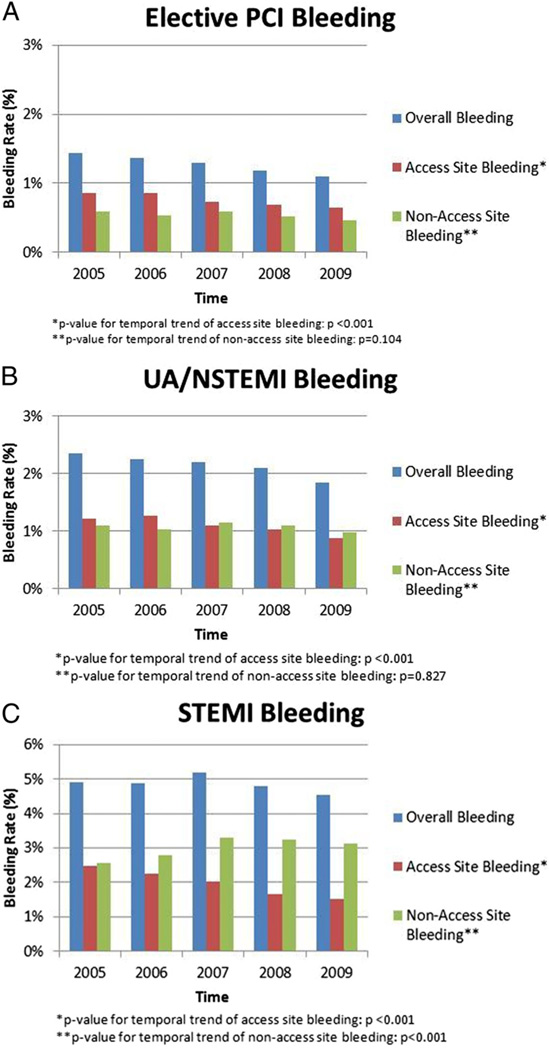
Objectives: The purpose of this study was to examine temporal trends in post-percutaneous coronary intervention (PCI) bleeding among patients with elective PCI, unstable angina (UA)/non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI).
Background: The impact of bleeding avoidance strategies on post-PCI bleeding rates over time is unknown.
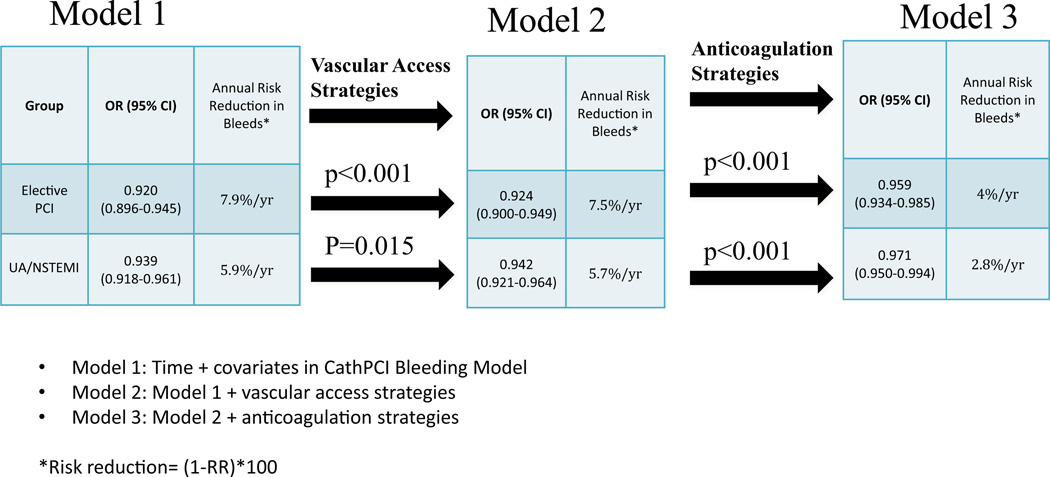
Methods: Using the CathPCI Registry, we examined temporal trends in post-PCI bleeding from 2005 to 2009 among patients with elective PCI (n = 599,524), UA/NSTEMI (n = 836,103), and STEMI (n = 267,632). We quantified the linear time trend in bleeding using 3 sequential logistic regression models: 1) clinical factors; 2) clinical + vascular access strategies (femoral vs. radial, use of closure devices); and 3) clinical, vascular strategies + antithrombotic treatments (anticoagulant ± glycoprotein IIb/IIIa inhibitor [GPI]). Changes in the odds ratio for time trend in bleeding were compared using bootstrapping and converted to risk ratio.
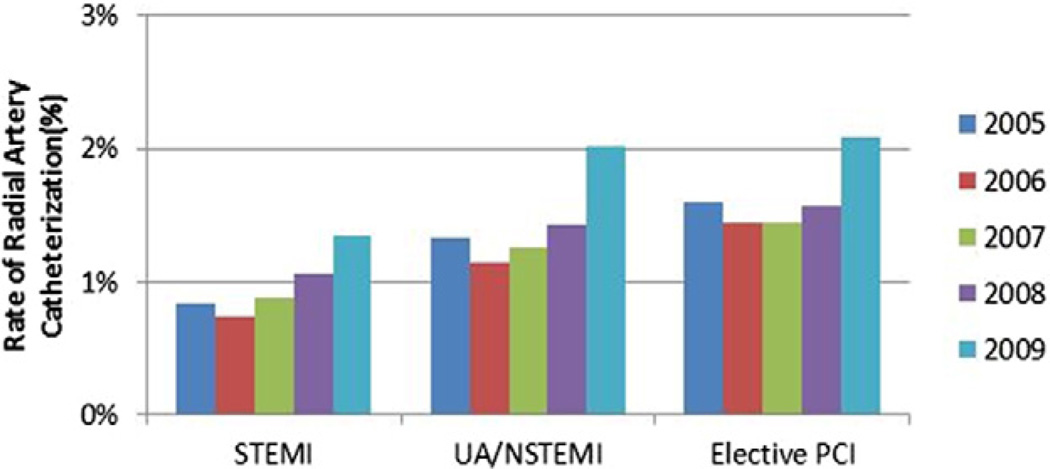
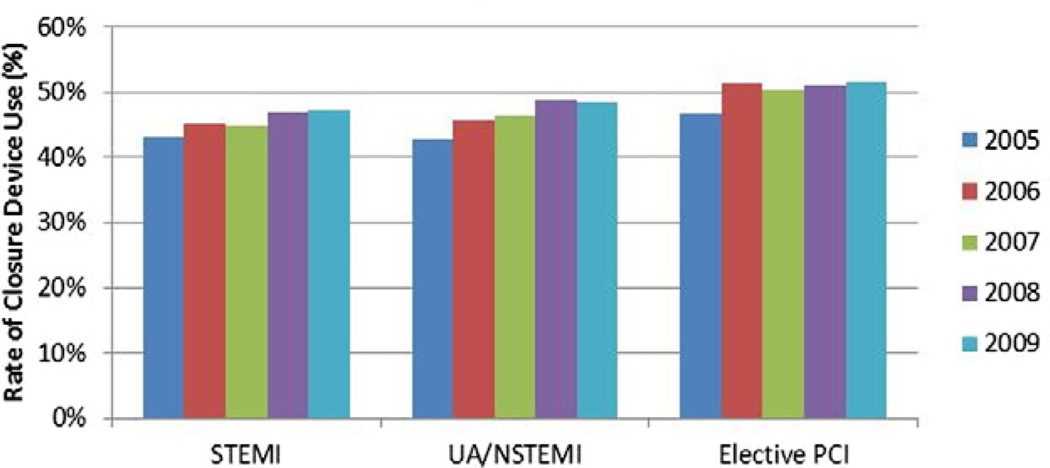
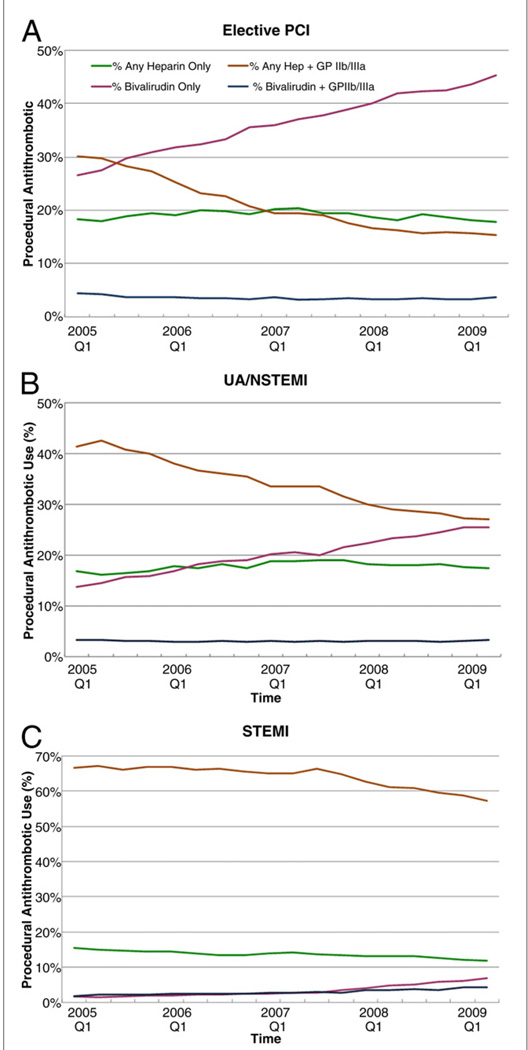
Results: An approximate 20% reduction in post-PCI bleeding was seen (elective PCI: 1.4% to 1.1%; UA/NSTEMI: 2.3% to 1.8; STEMI: 4.9% to 4.5%). Radial approach remained low (<3%), and closure device use increased marginally from 44% to 49%. Bivalirudin use increased (17% to 30%), whereas any heparin + GPI decreased (41% to 28%). There was a significant 6% to 8% per year reduction in annual bleeding risk in UA/NSTEMI and elective PCI, but not in STEMI. Antithrombotic strategies were associated with roughly half of the reduction in annual bleeding risk: change in risk ratio from 7.5% to 4% for elective PCI, and 5.7% to 2.8% for UA/NSTEMI (both p <0.001).
Conclusions: The nearly 20% reduction in post-PCI bleeding over time was largely due to temporal changes in antithrombotic strategies. Further reductions in bleeding complications may be possible as bleeding avoidance strategies evolve, especially in STEMI.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Eikelboom JW, Mehta SR, Anand SS, Xie C, Fox KA, Yusuf S. Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation. 2006;114:774–782. - PubMed
-
- Mehta SK, Frutkin AD, Lindsey JB, et al. Bleeding in patients undergoing percutaneous coronary intervention: the development of a clinical risk algorithm from the National Cardiovascular Data Registry. Circ Cardiovasc Interv. 2009;2:222–229. - PubMed
-
- Rao SV, Eikelboom JA, Granger CB, Harrington RA, Califf RM, Bassand JP. Bleeding and blood transfusion issues in patients with non-ST-segment elevation acute coronary syndromes. Eur Heart J. 2007;28:1193–1204. - PubMed
-
- Rao SV, Kaul PR, Liao L, et al. Association between bleeding, blood transfusion, and costs among patients with non-ST-segment elevation acute coronary syndromes. Am Heart J. 2008;155:369–374. - PubMed
-
- Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004;292:1555–1562. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
