

The role of autophagy in the pathogenesis of glycogen storage disease type II (GSDII)
- PMID: 22595755
- PMCID: PMC3438501
- DOI: 10.1038/cdd.2012.52
The role of autophagy in the pathogenesis of glycogen storage disease type II (GSDII)
Abstract
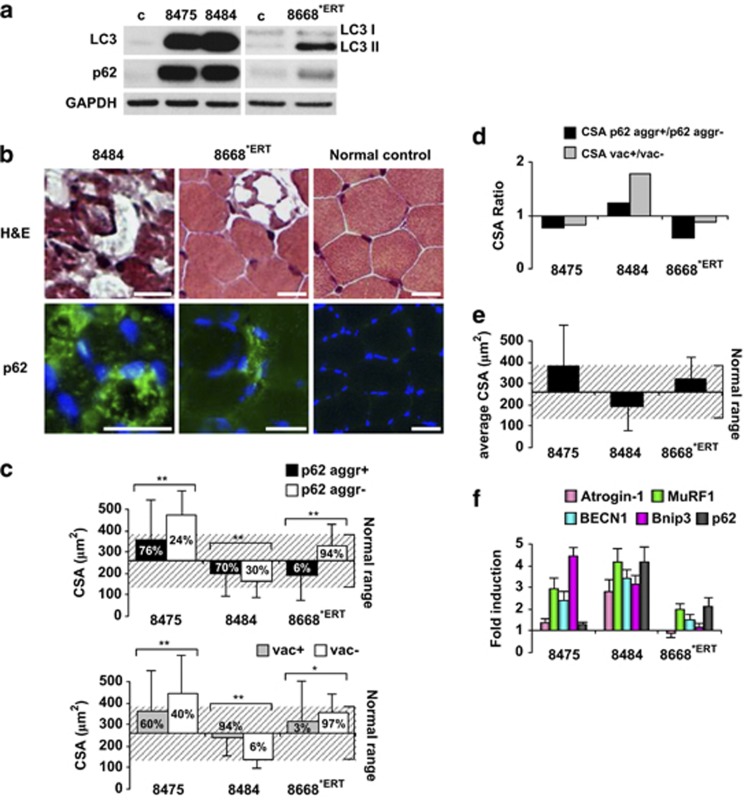
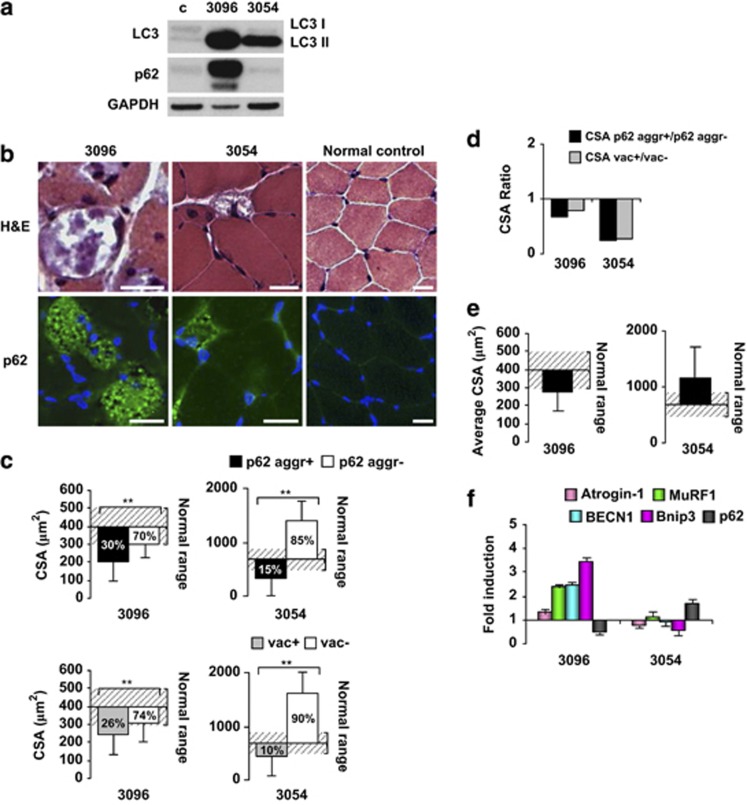
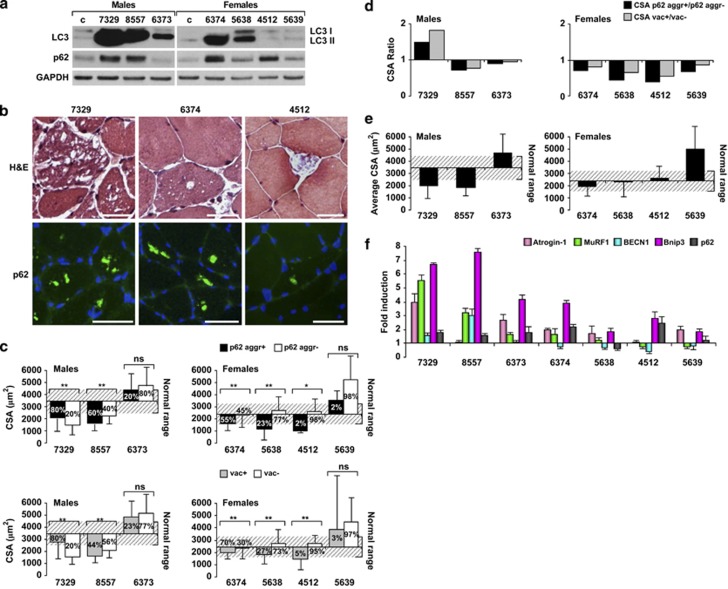
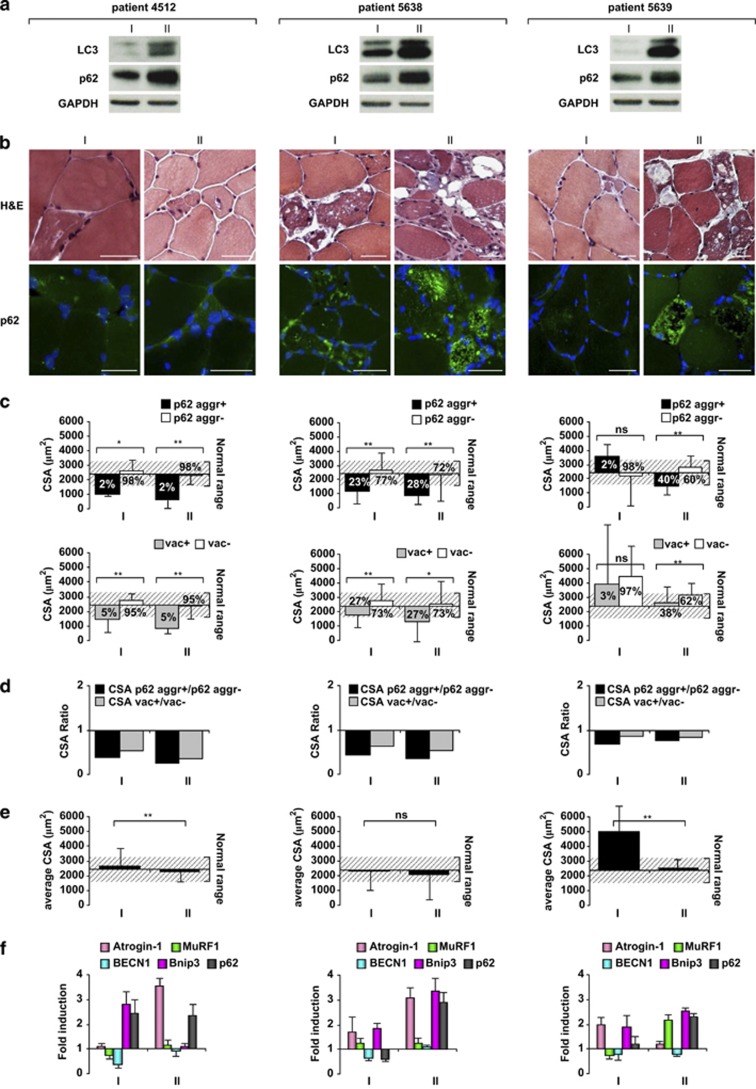
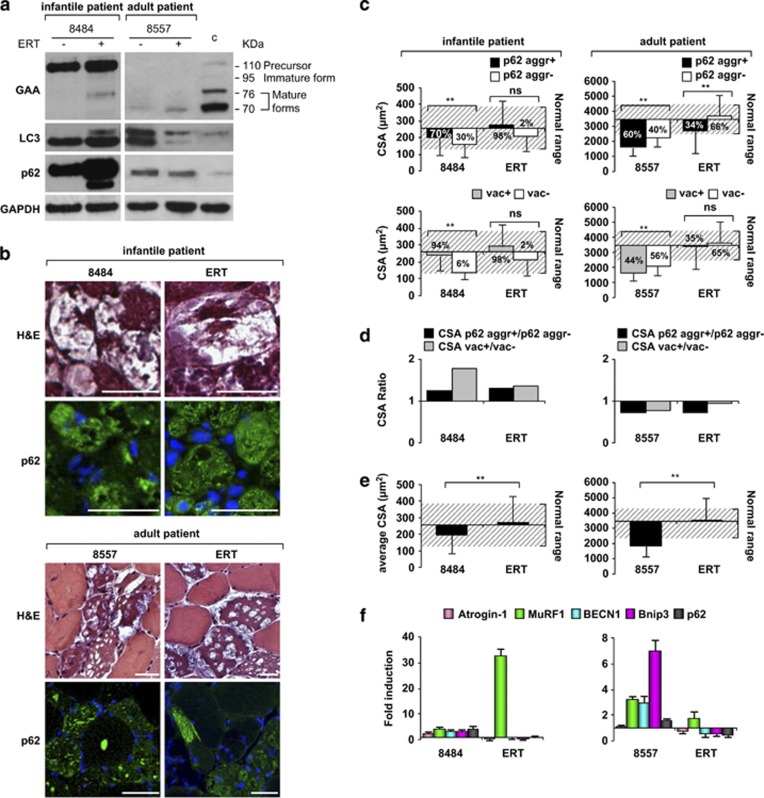
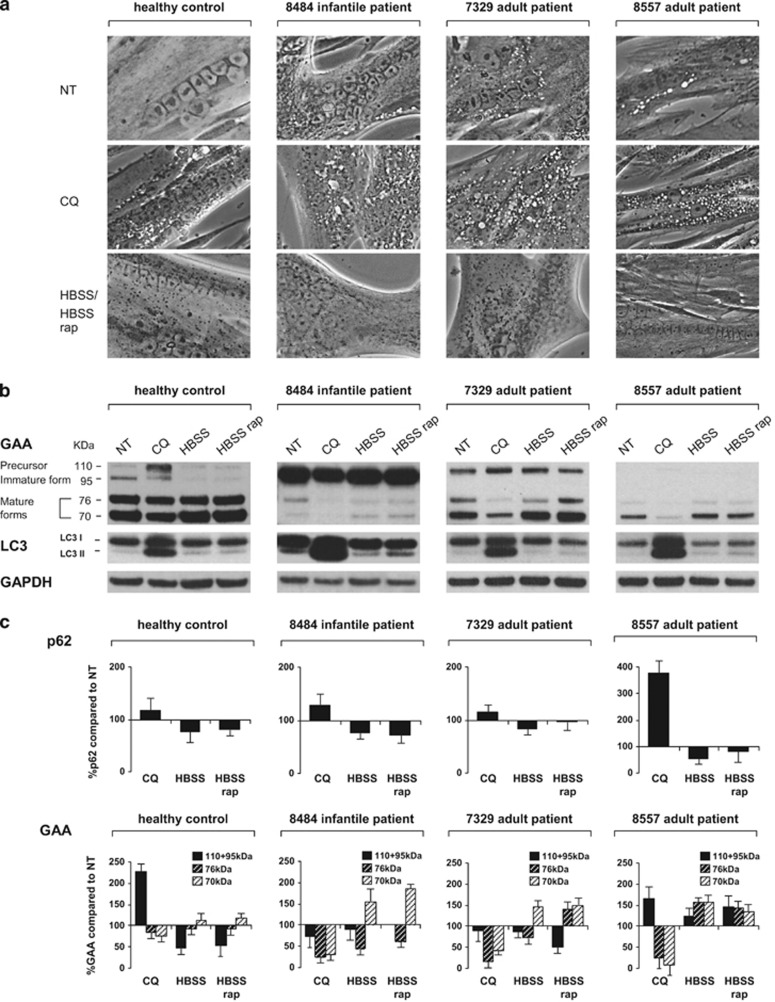
Regulated removal of proteins and organelles by autophagy-lysosome system is critical for muscle homeostasis. Excessive activation of autophagy-dependent degradation contributes to muscle atrophy and cachexia. Conversely, inhibition of autophagy causes accumulation of protein aggregates and abnormal organelles, leading to myofiber degeneration and myopathy. Defects in lysosomal function result in severe muscle disorders such as Pompe (glycogen storage disease type II (GSDII)) disease, characterized by an accumulation of autophagosomes. However, whether autophagy is detrimental or not in muscle function of Pompe patients is unclear. We studied infantile and late-onset GSDII patients and correlated impairment of autophagy with muscle wasting. We also monitored autophagy in patients who received recombinant α-glucosidase. Our data show that infantile and late-onset patients have different levels of autophagic flux, accumulation of p62-positive protein aggregates and expression of atrophy-related genes. Although the infantile patients show impaired autophagic function, the late-onset patients display an interesting correlation among autophagy impairment, atrophy and disease progression. Moreover, reactivation of autophagy in vitro contributes to acid α-glucosidase maturation in both healthy and diseased myotubes. Together, our data suggest that autophagy protects myofibers from disease progression and atrophy in late-onset patients.
Figures
References
-
- Mammucari C, Milan G, Romanello V, Masiero E, Rudolf R, Del Piccolo P, et al. FoxO3 controls autophagy in skeletal muscle in vivo. Cell Metab. 2007;6:458–471. - PubMed
-
- Engel AG, Hirschhorn R, Huie ML.Acid maltase deficiencyIn: Engel AG, Franzini-Armstrong C (eds).Myology McGraw-Hill Press: New York; 20041559–1586.
-
- Nishino I, Fu J, Tanji K, Yamada T, Shimojo S, Koori T, et al. Primary LAMP-2 deficiency causes X-linked vacuolar cardiomyopathy and myopathy (Danon disease) Nature. 2000;406:906–910. - PubMed
-
- Kalimo H, Savontaus ML, Lang H, Paljärvi L, Sonninen V, Dean PB, et al. X-linked myopathy with excessive autophagy: a new hereditary muscle disease. Ann Neurol. 1988;23:258–265. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
