

Performance of a multi-biomarker score measuring rheumatoid arthritis disease activity in the CAMERA tight control study
- PMID: 22596166
- PMCID: PMC3439649
- DOI: 10.1136/annrheumdis-2011-200963
Performance of a multi-biomarker score measuring rheumatoid arthritis disease activity in the CAMERA tight control study
Abstract
Objectives: To evaluate the performance of individual biomarkers and a multi-biomarker disease activity (MBDA) score in the early rheumatoid arthritis (RA) patient population from the computer assisted management in early rheumatoid arthritis (CAMERA) study.
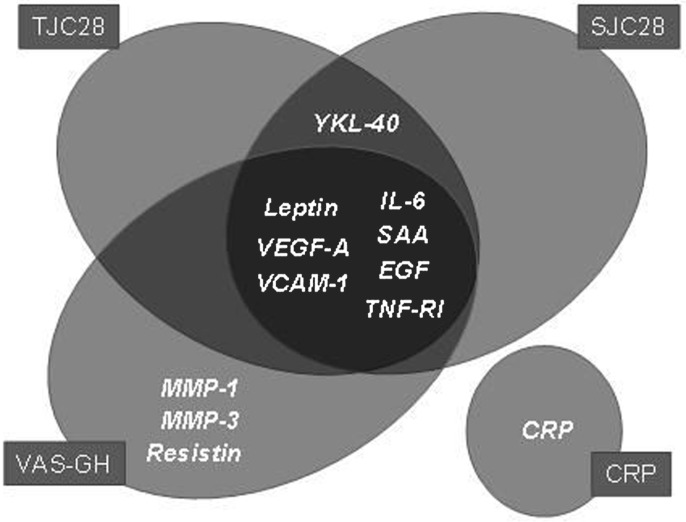
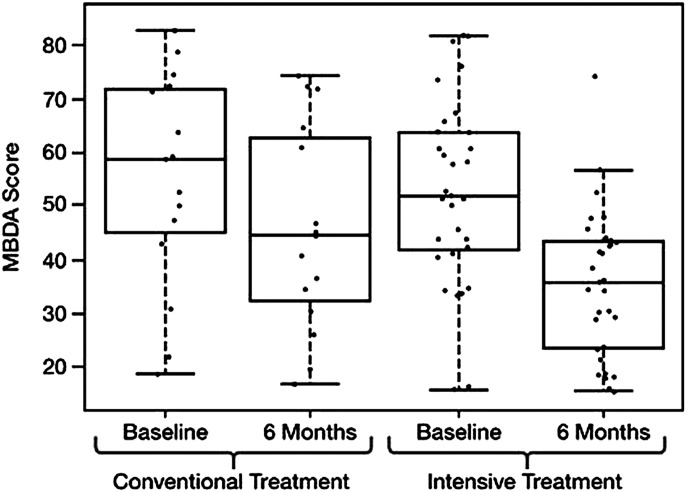
Methods: Twenty biomarkers were measured in the CAMERA cohort, in which patients were treated with either intensive or conventional methotrexate-based treatment strategies. The MBDA score was calculated using the concentrations of 12 biomarkers (SAA, IL-6, TNF-RI, VEGF-A, MMP-1, YKL-40, MMP-3, EGF, VCAM-1, leptin, resistin and CRP) according to a previously trained algorithm. The performance of the scores was evaluated relative to clinical disease activity assessments. Change in MBDA score over time was assessed by paired Wilcoxon rank sum test. Logistic regression was used to evaluate the ability of disease activity measures to predict radiographic progression.
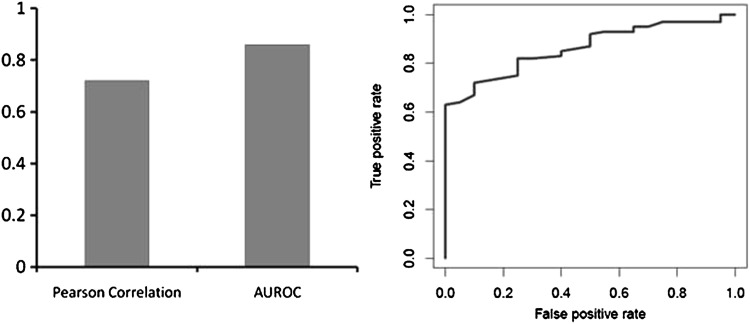
Results: The MBDA score had a significant correlation with the disease activity score based on 28 joints-C reactive protein (DAS28-CRP) (r=0.72; p<0.001) and an area under the receiver operating characteristic curve for distinguishing remission/low from moderate/high disease activity of 0.86 (p<0.001) using a DAS28-CRP cut-off of 2.7. In multivariate analysis the MBDA score, but not CRP, was an independent predictor of disease activity measures. Additionally, mean (SD) MBDA score decreased from 53 (18) at baseline to 39 (16) at 6 months in response to study therapy (p<0.0001). Neither MBDA score nor clinical variables were predictive of radiographic progression.
Conclusions: This multi-biomarker test performed well in the assessment of disease activity in RA patients in the CAMERA study. Upon further validation, this test could be used to complement currently available disease activity measures and improve patient care and outcomes.
Conflict of interest statement
Figures
References
-
- Kvien TK. Epidemiology and burden of illness of rheumatoid arthritis. Pharmacoeconomics 2004;22:1–12 - PubMed
-
- Atar D, Birkeland KI, Uhlig T. ‘Treat to target’: moving targets from hypertension, hyperlipidaemia and diabetes to rheumatoid arthritis. Ann Rheum Dis 2010;69:629–30 - PubMed
-
- Kiely PD, Brown AK, Edwards CJ, et al. Contemporary treatment principles for early rheumatoid arthritis: a consensus statement. Rheumatology (Oxford) 2009;48:765–72 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
