

Integrated rapid-diagnostic-test reader platform on a cellphone
- PMID: 22596243
- PMCID: PMC3390446
- DOI: 10.1039/c2lc40235a
Integrated rapid-diagnostic-test reader platform on a cellphone
Abstract
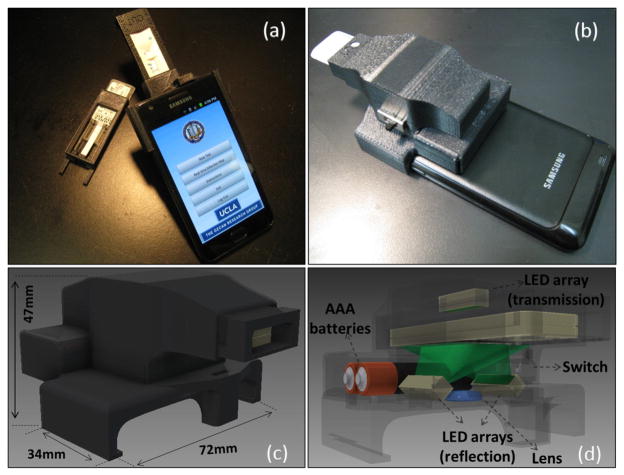
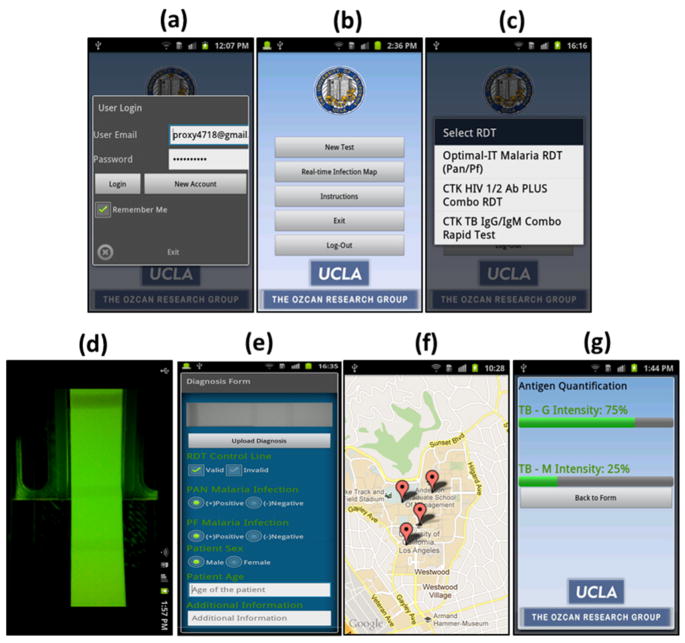
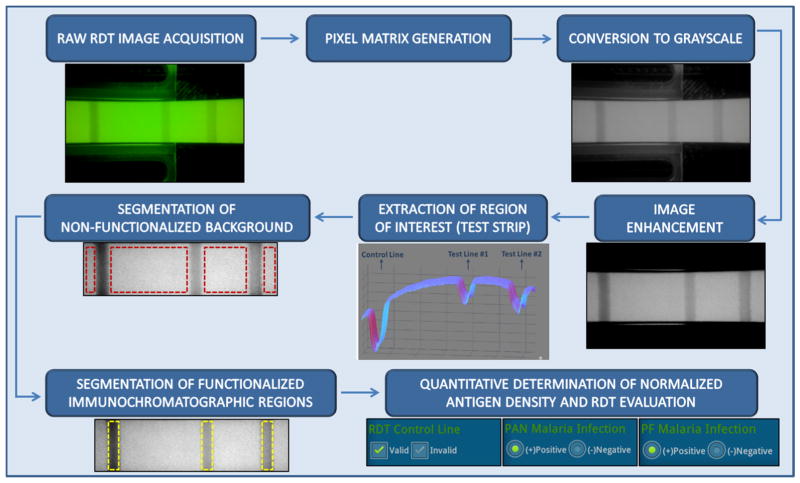
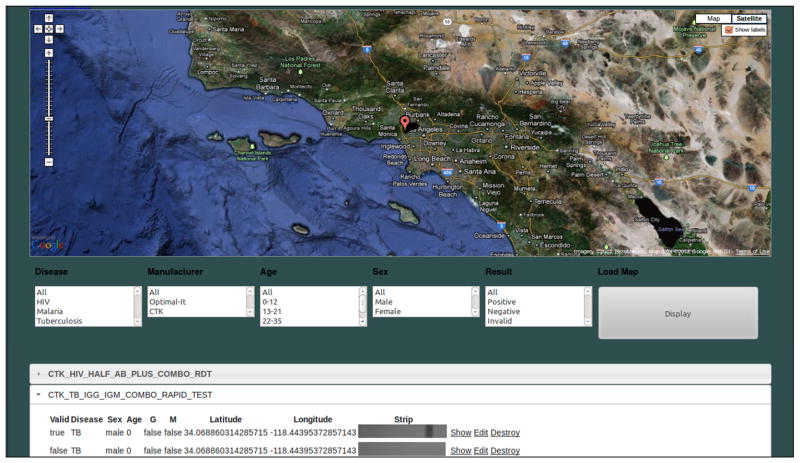
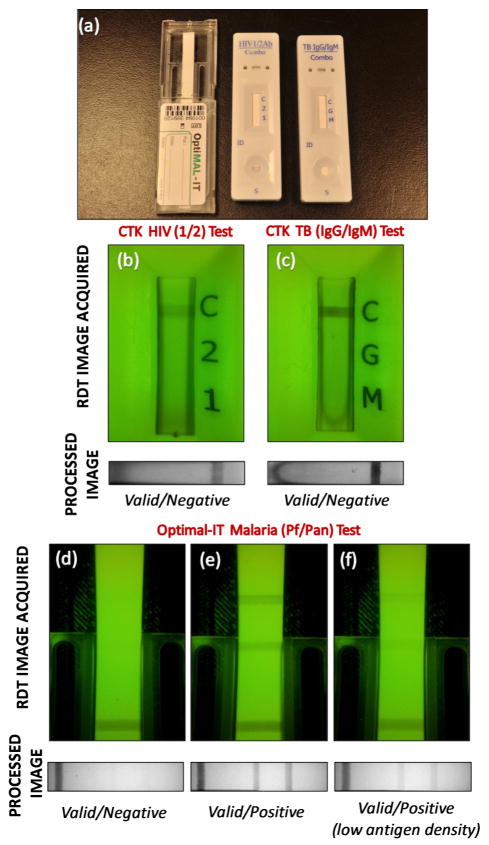
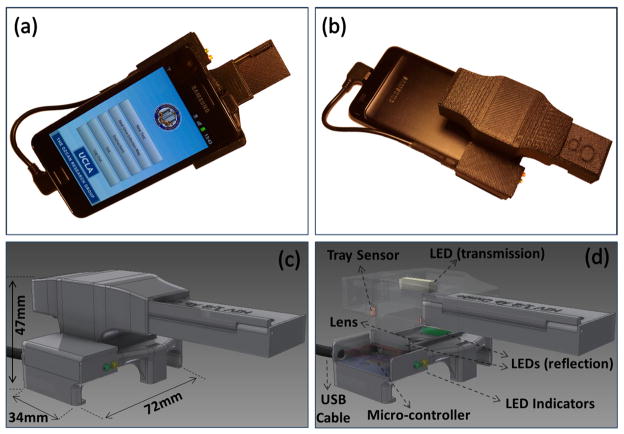
We demonstrate a cellphone-based rapid-diagnostic-test (RDT) reader platform that can work with various lateral flow immuno-chromatographic assays and similar tests to sense the presence of a target analyte in a sample. This compact and cost-effective digital RDT reader, weighing only ~65 g, mechanically attaches to the existing camera unit of a cellphone, where various types of RDTs can be inserted to be imaged in reflection or transmission modes under light-emitting diode (LED)-based illumination. Captured raw images of these tests are then digitally processed (within less than 0.2 s per image) through a smart application running on the cellphone for validation of the RDT, as well as for automated reading of its diagnostic result. The same smart application then transmits the resulting data, together with the RDT images and other related information (e.g., demographic data), to a central server, which presents the diagnostic results on a world map through geo-tagging. This dynamic spatio-temporal map of various RDT results can then be viewed and shared using internet browsers or through the same cellphone application. We tested this platform using malaria, tuberculosis (TB) and HIV RDTs by installing it on both Android-based smartphones and an iPhone. Providing real-time spatio-temporal statistics for the prevalence of various infectious diseases, this smart RDT reader platform running on cellphones might assist healthcare professionals and policymakers to track emerging epidemics worldwide and help epidemic preparedness.
Figures
References
-
- Banoo S, Bell D, Bossuyt P, Herring A, Mabey D, et al. Nat Rev Microbio. 2006;4:21–31.
-
- Wongsrichanalai C, Barcu MJ, Muth S, Sutamihardja A, Wernsdorfer WH. Am J Trop Med Hyg. 2007;77:119–127. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical