

Airway imaging in disease: gimmick or useful tool?
- PMID: 22604891
- PMCID: PMC3424064
- DOI: 10.1152/japplphysiol.00372.2012
Airway imaging in disease: gimmick or useful tool?
Abstract
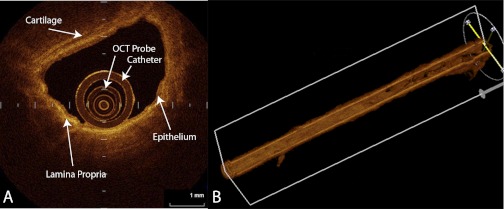
Airway remodeling is an important pathophysiological mechanism in a variety of chronic airway diseases. Historically investigators have had to use invasive techniques such as histological examination of excised tissue to study airway wall structure. The last several years has seen a proliferation of relatively noninvasive techniques to assess the airway branching pattern, wall thickness, and more recently, airway wall tissue components. These methods include computed tomography, magnetic resonance imaging, and optical coherence tomography. These new imaging technologies have become popular because to understand the physiology of lung disease it is important we understand the underlying anatomy. However, these new approaches are not standardized or available in all centers so a review of their validity and clinical utility is appropriate. This review documents how investigators are working hard to correct for inconsistencies between techniques so that they become more accepted and utilized in clinical settings. These new imaging techniques are very likely to play a frontline role in the study of lung disease and will, hopefully, allow clinicians and investigators to better understand disease pathogenesis and to design and assess new therapeutic interventions.
Figures
References
-
- Aldrich JE, Bilawich AM, Mayo JR. Radiation doses to patients receiving computed tomography examinations in British Columbia. Can Assoc Radiol J 57: 79–85, 2006 - PubMed
-
- Armstrong JJ, Leigh MS, Sampson DD, Walsh JH, Hillman DR, Eastwood PR. Quantitative upper airway imaging with anatomic optical coherence tomography. Am J Respir Crit Care Med 173: 226–233, 2006 - PubMed
-
- Armstrong JJ, Leigh MS, Walton ID, Zvyagin AV, Alexandrov SA, Schwer S, Sampson DD. In vivo size and shape measurement of the human upper airway using endoscopic long-range optical coherence tomography. Optics Express 2003: 1817–1826, 2003 - PubMed
-
- Bankier AA, Fleischmann D, Mallek R, Windisch A, Winkelbauer FW, Kontrus M, Havelec L, Herold CJ, Hubsch P. Bronchial wall thickness: Appropriate window settings for thin-section CT and radiologic-anatomic correlation. Radiology 199: 831–836, 1996 - PubMed
-
- Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, Gibson P, Ohta K, O'Byrne P, Pedersen SE, Pizzichini E, Sullivan SD, Wenzel SE, Zar HJ. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J 31: 143–178, 2008 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical