

Case Reports
doi: 10.1155/2011/121985.
Epub 2011 Sep 11.
Oncoplastic surgery in Japanese patients with breast cancer close to the areola: partial mastectomy using periareolar mammoplasty: a case report
Affiliations
- PMID: 22606571
- PMCID: PMC3350227
- DOI: 10.1155/2011/121985
Item in Clipboard
Case Reports
Oncoplastic surgery in Japanese patients with breast cancer close to the areola: partial mastectomy using periareolar mammoplasty: a case report
Case Rep Surg.
2011.
Abstract
We report the results of oncoplastic surgery in two Japanese patients with early breast cancer. Their breasts were large and ptotic, and their lesions, which were close to the areola, were considered to be suitable for breast conservative surgery. Oncoplastic surgery involving partial resection of the gland and a periareolar mammoplasty were performed. The technique was easy to perform, and the cosmetic outcome was excellent.
Figures

Case 1. A 51-year-old patient with a T1 tumor in the upper-inner area of her left breast. (a) Bilateral ptotic breasts with the nipple-areola complex (NAC) located beneath the inframammary line. The surgical scar produced by the excisional biopsy was located at the 11 O'clock position of her left breast. (b) Cystic degeneration caused by the excision biopsy was detected by ultrasonography. Periareolar mammaplasty was planned. (c) Postoperative 18 months.

Preoperative design of the periareolar technique showing the tumor. (a) A crescent of skin was removed together with a partial gland. A residual cancer lesion was suspected (red circle). (b) A cylinder of gland tissue was removed together with the pectoralis major muscle. (c) A suction tube was left on the surface of pectoral major muscle. (d) The superior and inferior pedicles were sutured to reduce the defect. (e) The areola suturing was completed with a single suture 4-0 PDS and a running subcuticular 4-0 Monocryl. (f) After closure.
Pre- and postoperative images of case 1. (a) A crescent of skin and the parenchymal tissue just under it were removed. (b) Identical bilateral procedures were performed.

Bilateral resected tissue. (a) The resected tissues weighed 94 g (right) and 104 g (left), respectively. (b) Fixed and sliced tissue used for the histological examination. No residual cancer cells were seen in the left breast.

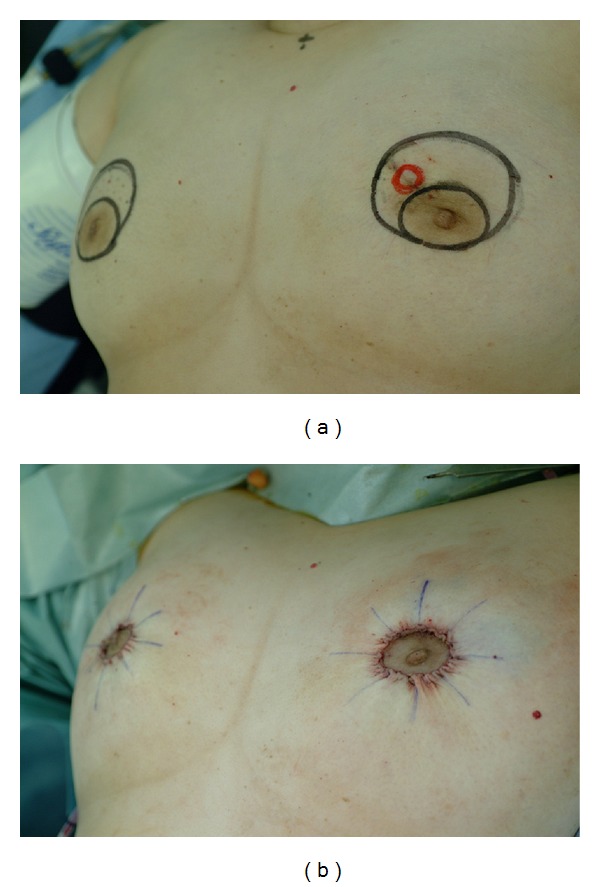
Case 2. a 51-year-old patient with a T1 tumor in the periareolar area of her left breast. (a) Her breasts were ptotic and large. (b) Lesions were detected by ultrasonography with the patient in a supine position. A 2 cm surgical margin (black circle) was drawn around the cancer lesion (red circle). No contralateral procedure was planned. (c) Postoperative 6 months.
References
-
- Audretsch WP, Rezai M, Kolotas C, Zamboglou N, Schnabel T, Bojar H. Tumor-specific immediate reconstruction in breast cancer patients. Perspectives in Plastic Surgery. 1998;11:71–106.
-
- Masetti R, Pirulli PG, Magno S, Franceschini G, Chiesa F, Antinori A. Oncoplastic techniques in the conservative surgical treatment of breast cancer. Breast Cancer. 2000;7(4):276–280. - PubMed
-
- Fitoussi A. Oncoplastic breast surgery. In: Fitoussi A, Berry MG, Couturaud B, Salmon RJ, editors. Oncoplastic and Reconstructive Surgery for Breast Cancer. Berlin, Germany: Springer; 2009. pp. 17–42.
-
- Berry MG, Fitoussi AD, Curnier B, Couturaud B, Salmon RJ. Oncoplastic breast surgery: a review and systematic approach. Journal of Plastic, Reconstructive and Aesthetic Surgery. 2010;63(8):1233–1243. - PubMed
-
- Audretsch WP, Rezai M, Kolotas C, Zamboglou N, Schnabel T, Bojar H. Onco-plastic surgery: “target” volume reduction (BCT-mastopexy), lumpectomy reconstruction (BCT-reconstruction) and flap-supported operability in breast cancer. In: Proceedings of the 2nd European Congress on Senology; October 1994; Vienna, Austria; Moncuzzi, Bologna, Italy. pp. 139–157.
Publication types
LinkOut - more resources
Full Text Sources
