

Minimizing risk of nephrogenic systemic fibrosis in cardiovascular magnetic resonance
- PMID: 22607376
- PMCID: PMC3409035
- DOI: 10.1186/1532-429X-14-31
Minimizing risk of nephrogenic systemic fibrosis in cardiovascular magnetic resonance
Abstract
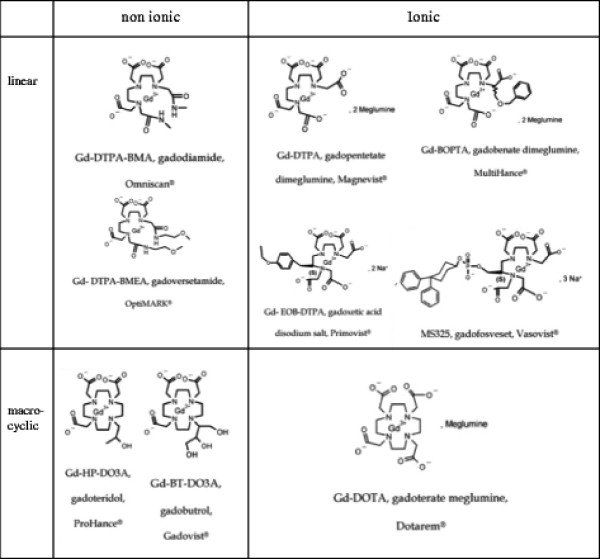
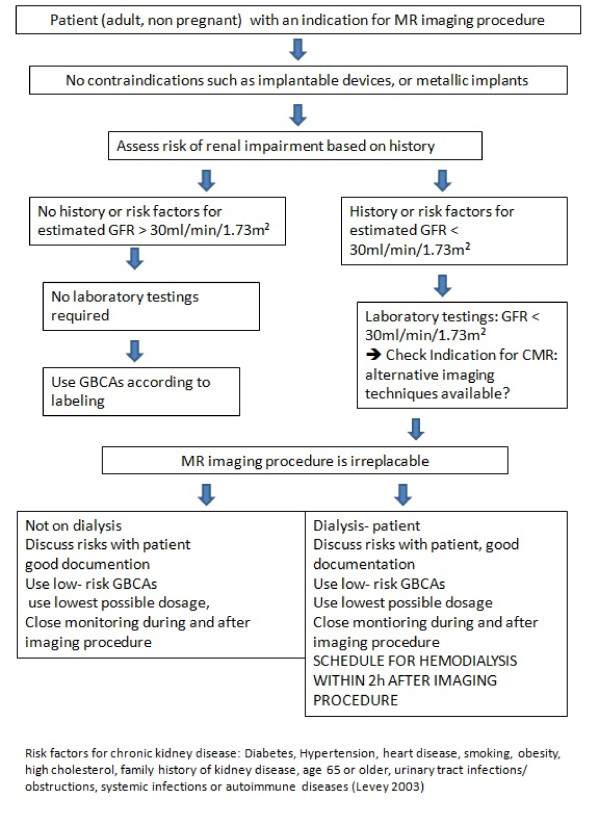
Nephrogenic Systemic Fibrosis is a rare condition appearing only in patients with severe renal impairment or failure and presents with dermal lesions and involvement of internal organs. Although many cases are mild, an estimated 5% have a progressive debilitating course. To date, there is no known effective treatment thus stressing the necessity of ample prevention measures. An association with the use of Gadolinium based contrast agents (GBCA) makes Nephrogenic Systemic Fibrosis a potential side effect of contrast enhanced magnetic resonance imaging and offers the opportunity for prevention by limiting use of gadolinium based contrast agents in renal failure patients. In itself toxic, Gadolinium is embedded into chelates that allow its safe use as a contrast agent. One NSF theory is that Gadolinium chelates distribute into the extracellular fluid compartment and set Gadolinium ions free, depending on multiple factors among which the duration of chelates exposure is directly related to the renal function. Major medical societies both in Europe and in North America have developed guidelines for the usage of GBCA. Since the establishment of these guidelines and the increased general awareness of this condition, the occurrence of NSF has been nearly eliminated. Giving an overview over the current knowledge of NSF pathobiochemistry, pathogenesis and treatment options this review focuses on the guidelines of the European Medicines Agency, the European Society of Urogenital Radiology, the FDA and the American College of Radiology from 2008 up to 2011 and the transfer of this knowledge into every day practice.
Figures
References
-
- The European Cardiovascular Magnetic Resonance Registry. www.eurocmr-registry.com.
-
- Idee JM. et al. Possible involvement of gadolinium chelates in the pathophysiology of nephrogenic systemic fibrosis: a critical review. Toxicology. 2008;248(2–3):77–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
