

Local electrogram delay recorded from left ventricular lead at implant predicts response to cardiac resynchronization therapy: retrospective study with 1 year follow up
- PMID: 22607487
- PMCID: PMC3447687
- DOI: 10.1186/1471-2261-12-34
Local electrogram delay recorded from left ventricular lead at implant predicts response to cardiac resynchronization therapy: retrospective study with 1 year follow up
Abstract
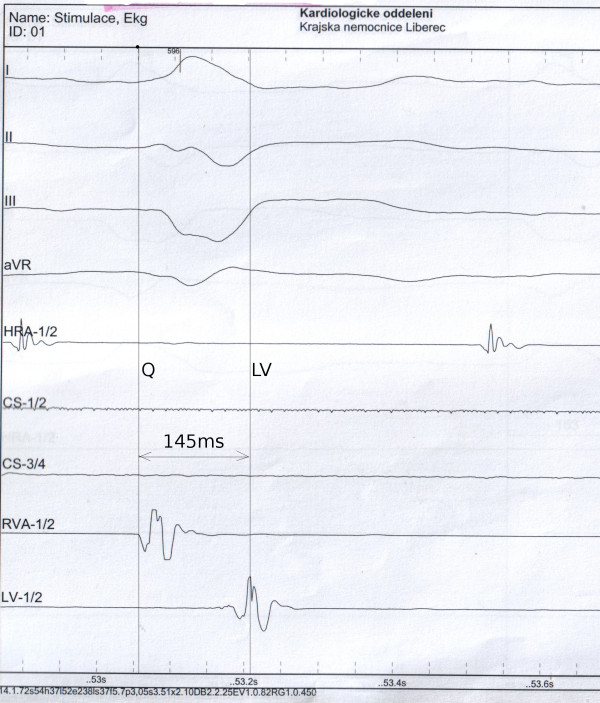
Background: Considerable proportion of patients does not respond to the cardiac resynchronization therapy (CRT). This study investigated clinical relevance of left ventricular electrode local electrogram delay from the beginning of QRS (QLV). We hypothesized that longer QLV indicating more optimal lead placement in the late activated regions is associated with the higher probability of positive CRT response.
Methods: We conducted a retrospective, single-centre analysis of 161 consecutive patients with heart failure and LBBB or nonspecific intraventricular conduction delay (IVCD) treated with CRT. We routinely intend to implant the LV lead in a region with long QLV. Clinical response to CRT, left ventricular (LV) reverse remodelling (i.e. decrease in LV end-systolic diameter - LVESD ≥10%) and reduction in plasma level of NT-proBNP >30% at 12-month post-implant were the study endpoints. We analyzed association between pre-implant variables and the study endpoints.
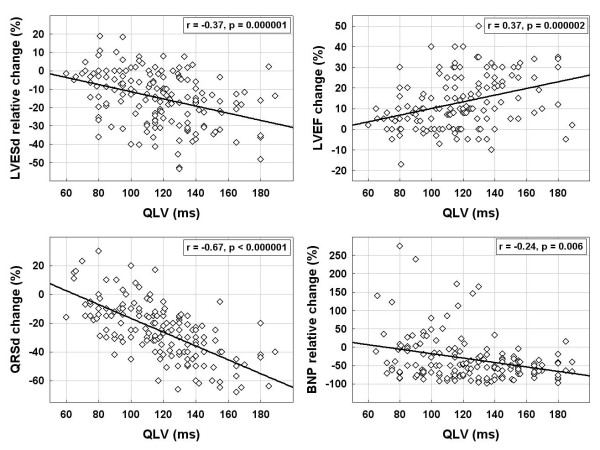
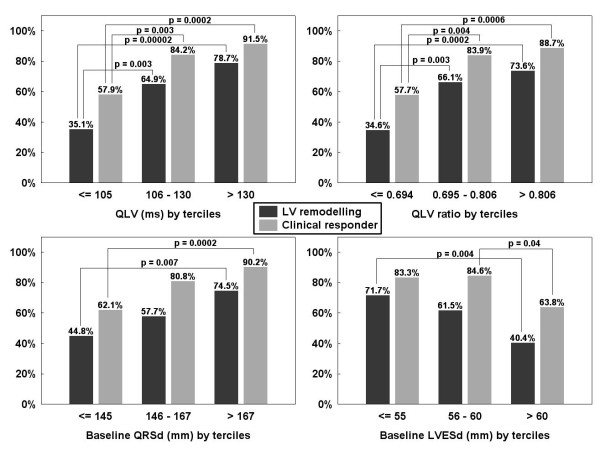
Results: Clinical CRT response rate reached 58%, 84% and 92% in the lowest (≤105 ms), middle (106-130 ms) and the highest (>130 ms) QLV tertile (p < 0.0001), respectively. Longer QRS duration (p = 0.002), smaller LVESD and a non-ischemic cardiomyopathy (both p = 0.02) were also univariately associated with positive clinical CRT response. In a multivariate analysis, QLV remained the strongest predictor of clinical CRT response (p < 0.00001), followed by LVESD (p = 0.01) and etiology of LV dysfunction (p = 0.04). Comparable predictive power of QLV for LV reverse remodelling and NT-proBNP response rates was observed.
Conclusion: LV lead position assessed by duration of the QLV interval was found the strongest independent predictor of beneficial clinical response to CRT.
Figures
References
-
- Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG. et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350(21):2140–2150. doi: 10.1056/NEJMoa032423. - DOI - PubMed
-
- Linde C, Abraham WT, Gold MR. St John Sutton M, Ghio S, Daubert C: Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008;52(23):1834–1843. doi: 10.1016/j.jacc.2008.08.027. - DOI - PubMed
-
- Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, Garrigue S, Kappenberger L, Haywood GA, Santini M. et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001;344(12):873–880. doi: 10.1056/NEJM200103223441202. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
