

Effects of tailored neck-shoulder pain treatment based on a decision model guided by clinical assessments and standardized functional tests. A study protocol of a randomized controlled trial
- PMID: 22607546
- PMCID: PMC3517365
- DOI: 10.1186/1471-2474-13-75
Effects of tailored neck-shoulder pain treatment based on a decision model guided by clinical assessments and standardized functional tests. A study protocol of a randomized controlled trial
Abstract
Background: A major problem with rehabilitation interventions for neck pain is that the condition may have multiple causes, thus a single treatment approach is seldom efficient. The present study protocol outlines a single blinded randomised controlled trial evaluating the effect of tailored treatment for neck-shoulder pain. The treatment is based on a decision model guided by standardized clinical assessment and functional tests with cut-off values. Our main hypothesis is that the tailored treatment has better short, intermediate and long-term effects than either non-tailored treatment or treatment-as-usual (TAU) on pain and function. We sub-sequentially hypothesize that tailored and non-tailored treatment both have better effect than TAU.
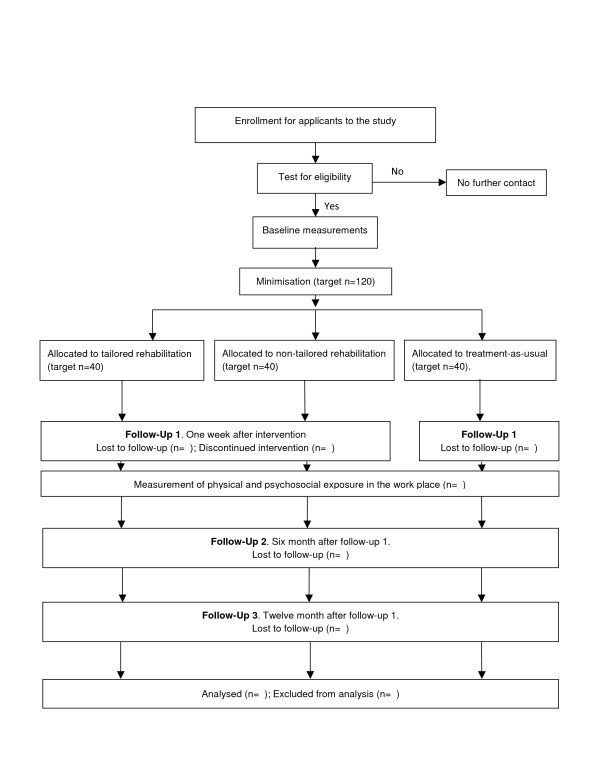
Methods/design: 120 working women with minimum six weeks of nonspecific neck-shoulder pain aged 20-65, are allocated by minimisation with the factors age, duration of pain, pain intensity and disability in to the groups tailored treatment (T), non-tailored treatment (NT) or treatment-as-usual (TAU). Treatment is given to the groups T and NT for 11 weeks (27 sessions evenly distributed). An extensive presentation of the tests and treatment decision model is provided. The main treatment components are manual therapy, cranio-cervical flexion exercise and strength training, EMG-biofeedback training, treatment for cervicogenic headache, neck motor control training. A decision algorithm based on the baseline assessment determines the treatment components given to each participant of T- and NT-groups. Primary outcome measures are physical functioning (Neck Disability Index) and average pain intensity last week (Numeric Rating Scale). Secondary outcomes are general improvement (Patient Global Impression of Change scale), symptoms (Profile Fitness Mapping neck questionnaire), capacity to work in the last 6 weeks (quality and quantity) and pressure pain threshold of m. trapezius. Primary and secondary outcomes will be reported for each group with effect size and its precision.
Discussion: We have chosen not to include women with psychological ill-health and focus on biomedical aspects of neck pain. Future studies should aim at including psychosocial aspects in a widened treatment decision model. No important adverse events or side-effects are expected.
Figures


References
-
- Gross AR, Goldsmith C, Hoving JL, Haines T, Peloso P, Aker P, Santaguida P, Myers C. Conservative management of mechanical neck disorders: a systematic review. J Rheumatol. 2007;34:1083–1102. - PubMed
-
- Hurwitz EL, Carragee EJ, van der Velde G, Carroll LJ, Nordin M, Guzman J, Peloso PM, Holm LW, Cote P, Hogg-Johnson S. et al.Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976) 2008;33:S123–152. doi: 10.1097/BRS.0b013e3181644b1d. - DOI - PubMed
-
- Kay TM, Gross A, Goldsmith C, Santaguida PL, Hoving J, Bronfort G, Cervical Overview G. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. 2005. p. CD004250. - PubMed
-
- SBU. Metoder för behandling av långvarig smärta : en systematisk litteraturöversikt. Stockholm Statens beredning för medicinsk utvärdering (SBU) 2006;1:159.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
