

Does access to a colorectal cancer screening website and/or a nurse-managed telephone help line provided to patients by their family physician increase fecal occult blood test uptake?: A pragmatic cluster randomized controlled trial study protocol
- PMID: 22607726
- PMCID: PMC3495851
- DOI: 10.1186/1471-2407-12-182
Does access to a colorectal cancer screening website and/or a nurse-managed telephone help line provided to patients by their family physician increase fecal occult blood test uptake?: A pragmatic cluster randomized controlled trial study protocol
Abstract
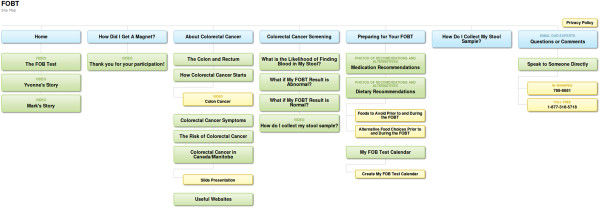
Background: Fecal occult blood test screening in Canada is sub-optimal. Family physicians play a central role in screening and are limited by the time constraints of clinical practice. Patients face multiple barriers that further reduce completion rates. Tools that support family physicians in providing their patients with colorectal cancer information and that support uptake may prove useful. The primary objective of the study is to evaluate the efficacy of a patient decision aid (nurse-managed telephone support line and/or colorectal cancer screening website) distributed by community-based family physicians, in improving colorectal cancer screening rates. Secondary objectives include evaluation of (dis)incentives to patient FOBT uptake and internet use among 50 to 74 year old males and females for health-related questions. Challenges faced by family physicians in engaging in collaborative partnerships with primary healthcare researchers will be documented.
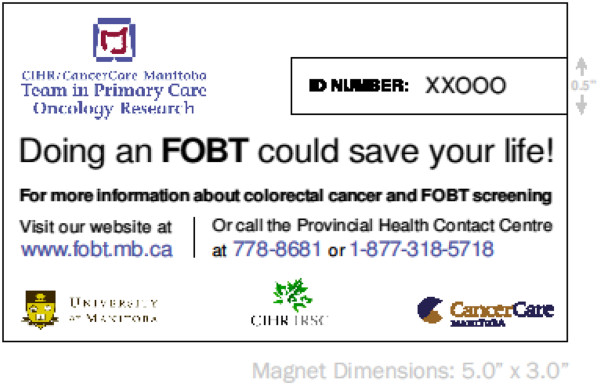
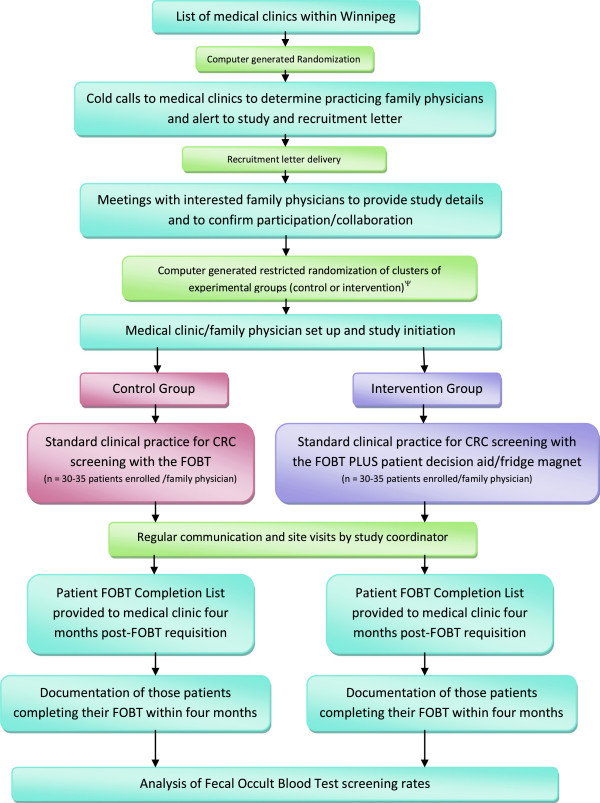
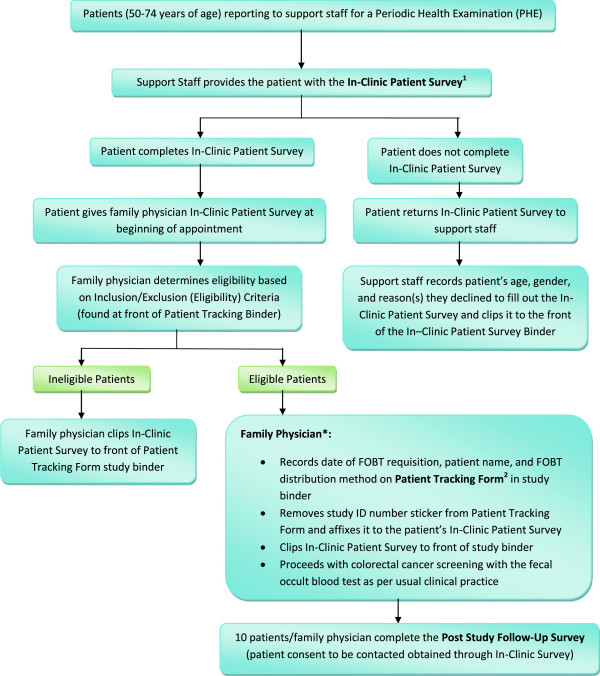
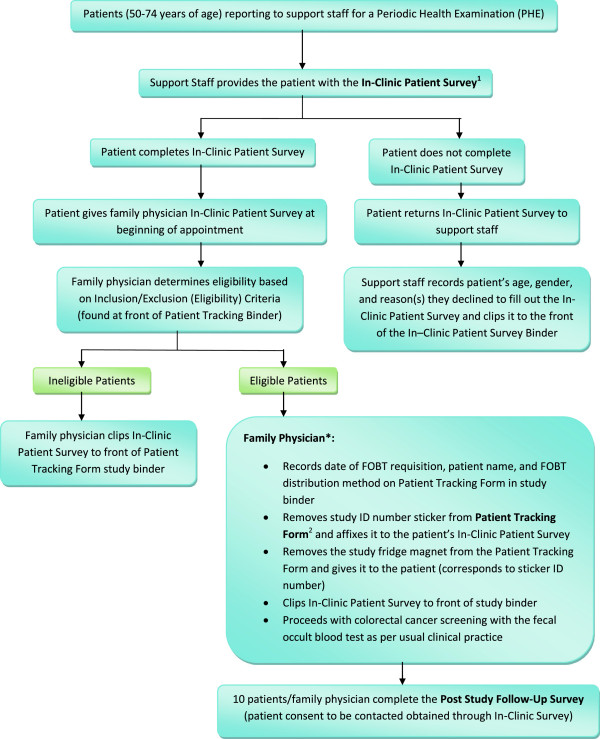
Methods/design: A pragmatic, two-arm, randomized cluster controlled trial conducted in 22 community-based family practice clinics (36 clusters) with 76 fee-for-service family physicians in Winnipeg, Manitoba, Canada. Each physician will enroll 30 patients attending their periodic health examination and at average risk for colorectal cancer. All physicians will follow their standard clinical practice for screening. Intervention group physicians will provide a fridge magnet to each patient that contains information facilitating access to the study-specific colorectal cancer screening decision aids (telephone help-line and website). The primary endpoint is patient fecal occult blood test completion rate after four months (intention to treat model). Multi-level analysis will include clinic, physician and patient level variables. Patient Personal Health Identification Numbers will be collected from those providing consent to facilitate analysis of repeat screening behavior. Secondary outcome data will be obtained through the Clinic Characterization Form, Patient Tracking Form, In-Clinic Patient Survey, Post-Study Follow-Up Patient Survey, and Family Physician Survey. Study protocol approved by The University of Manitoba Health Research Ethics Board.
Discussion: The study intervention has the potential to increase patient fecal occult blood test uptake, decrease colorectal cancer mortality and morbidity, and improve the health of Manitobans. If utilization of the website and/or telephone support line result in clinically significant increases in colorectal cancer screening uptake, changes in screening at the policy- and system-level may be warranted.
Trial registration: Clinical trials.gov identifier NCT01026753.
Figures
Similar articles
-
Does access to a colorectal cancer screening website and/or a nurse-managed telephone help line provided to patients by their family physician increase fecal occult blood test uptake?: results from a pragmatic cluster randomized controlled trial.BMC Cancer. 2014 Apr 16;14:263. doi: 10.1186/1471-2407-14-263. BMC Cancer. 2014. PMID: 24739235 Free PMC article. Clinical Trial.
-
Comparing the effect of a decision aid plus patient navigation with usual care on colorectal cancer screening completion in vulnerable populations: study protocol for a randomized controlled trial.Trials. 2014 Jul 8;15:275. doi: 10.1186/1745-6215-15-275. Trials. 2014. PMID: 25004983 Free PMC article. Clinical Trial.
-
Virtual colonoscopy, optical colonoscopy, or fecal occult blood testing for colorectal cancer screening: results of a pilot randomized controlled trial.Trials. 2015 Jul 9;16:296. doi: 10.1186/s13063-015-0826-7. Trials. 2015. PMID: 26156248 Free PMC article. Clinical Trial.
-
Peer Support as an Ideal Solution for Racial/Ethnic Disparities in Colorectal Cancer Screening: Evidence from a Systematic Review and Meta-analysis.Dis Colon Rectum. 2020 Jun;63(6):850-858. doi: 10.1097/DCR.0000000000001611. Dis Colon Rectum. 2020. PMID: 32167969
-
Colorectal cancer screening: why immunochemical fecal occult blood tests may be the best option.BMC Gastroenterol. 2012 Dec 29;12:183. doi: 10.1186/1471-230X-12-183. BMC Gastroenterol. 2012. PMID: 23272939 Free PMC article. Review.
Cited by
-
Reporting of sex and gender in randomized controlled trials in Canada: a cross-sectional methods study.Res Integr Peer Rev. 2017 Sep 1;2:15. doi: 10.1186/s41073-017-0039-6. eCollection 2017. Res Integr Peer Rev. 2017. PMID: 29451565 Free PMC article.
-
Evaluation of a service intervention to improve awareness and uptake of bowel cancer screening in ethnically-diverse areas.Br J Cancer. 2014 Sep 23;111(7):1440-7. doi: 10.1038/bjc.2014.363. Epub 2014 Jul 1. Br J Cancer. 2014. PMID: 24983374 Free PMC article.
-
Does access to a colorectal cancer screening website and/or a nurse-managed telephone help line provided to patients by their family physician increase fecal occult blood test uptake?: results from a pragmatic cluster randomized controlled trial.BMC Cancer. 2014 Apr 16;14:263. doi: 10.1186/1471-2407-14-263. BMC Cancer. 2014. PMID: 24739235 Free PMC article. Clinical Trial.
References
-
- Canadian Cancer Society. Canadian Cancer Society: Canadian Cancer Statistics, 2011. Toronto; 2011. [ http://www.cancer.ca]
-
- Canadian Partnership Against Cancer. Colorectal Screening in Canada: Current Facts and Resources. Resource Library; October, 2010. [ http://www.cancerview.ca.]
-
- PRA Inc. Colorectal cancer screening: Results of a survey of Manitobans 50–74. Manitoba; 2008. [ http://www.cancercare.mb.ca/resource/File/CRC/Background_ColonCheck_Mani...]
-
- Statistics Canada. Study: Mammography use and colorectal cancer testing. 2009. [ http://www.statcan.gc.ca/daily-quotidien/090630/dq090630c-eng.htm]
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
