

Physical function and independence 1 year after myocardial infarction: observations from the Translational Research Investigating Underlying disparities in recovery from acute Myocardial infarction: Patients' Health status registry
- PMID: 22607856
- PMCID: PMC3359897
- DOI: 10.1016/j.ahj.2012.02.024
Physical function and independence 1 year after myocardial infarction: observations from the Translational Research Investigating Underlying disparities in recovery from acute Myocardial infarction: Patients' Health status registry
Abstract
Background: Acute myocardial infarction (AMI) may contribute to health status declines including "independence loss" and "physical function decline." Despite the importance of these outcomes for prognosis and quality of life, their incidence and predictors have not been well described.
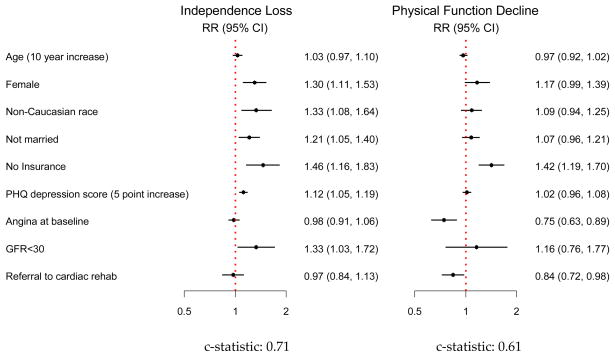
Methods: We studied 2,002 patients with AMI enrolled across 24 sites in the TRIUMPH registry who completed assessments of independence and physical function at the time of AMI and 1 year later. Independence was evaluated by the EuroQol-5D (mobility, self-care, and usual activities), and physical function was assessed with the Short Form-12 physical component score. Declines in ≥1 level on EuroQol-5D and >5 points in PCS were considered clinically significant changes. Hierarchical, multivariable, modified Poisson regression models accounting for within-site variability were used to identify predictors of independence loss and physical function decline.
Results: One-year post AMI, 43.0% of patients experienced health status declines: 12.8% independence loss alone, 15.2% physical function decline alone, and 15.0% both. After adjustment, variables that predicted independence loss included female sex, nonwhite race, unmarried status, uninsured status, end-stage renal disease, and depression. Variables that predicted physical function decline were uninsured status, lack of cardiac rehabilitation referral, and absence of pre-AMI angina. Age was not predictive of either outcome after adjustment.
Conclusions: >40% of patients experience independence loss or physical function decline 1 year after AMI. These changes are distinct but can occur simultaneously. Although some risk factors are not modifiable, others suggest potential targets for strategies to preserve patients' health status.
Copyright © 2012 Mosby, Inc. All rights reserved.
Figures
References
-
- Institute of Medicine. Crossing the quality chasm: A new health system for the 21st century. Washington, D.C.: National Academy Press; 2001. - PubMed
-
- Spertus JA. Evolving applications for patient-centered health status measures. Circulation. 2008;118:2103–10. - PubMed
-
- Ades PA, Savage PD, Tischler MD, et al. Determinants of disability in older coronary patients. Am Heart J. 2002;143:151–6. - PubMed
-
- Kamper AM, Stott DJ, Hyland M, et al. Predictors of functional decline in elderly people with vascular risk factors or disease. Age Ageing. 2005;34:450–5. - PubMed
-
- Alexander KP, Newby LK, Cannon CP, et al. Acute coronary care in the elderly, part I: Non-ST-segment-elevation acute coronary syndromes: A scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: In collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115:2549–69. - PubMed
