

Dabrafenib in patients with melanoma, untreated brain metastases, and other solid tumours: a phase 1 dose-escalation trial
- PMID: 22608338
- PMCID: PMC4109288
- DOI: 10.1016/S0140-6736(12)60398-5
Dabrafenib in patients with melanoma, untreated brain metastases, and other solid tumours: a phase 1 dose-escalation trial
Abstract
Background: Dabrafenib is an inhibitor of BRAF kinase that is selective for mutant BRAF. We aimed to assess its safety and tolerability and to establish a recommended phase 2 dose in patients with incurable solid tumours, especially those with melanoma and untreated, asymptomatic brain metastases.
Methods: We undertook a phase 1 trial between May 27, 2009, and March 20, 2012, at eight study centres in Australia and the USA. Eligible patients had incurable solid tumours, were 18 years or older, and had adequate organ function. BRAF mutations were mandatory for inclusion later in the study because of an absence of activity in patients with wild-type BRAF. We used an accelerated dose titration method, with the first dose cohort receiving 12 mg dabrafenib daily in a 21-day cycle. Once doses had been established, we expanded the cohorts to include up to 20 patients. On the basis of initial data, we chose a recommended phase 2 dose. Efficacy at the recommended phase 2 dose was studied in patients with BRAF-mutant tumours, including those with non-Val600Glu mutations, in three cohorts: metastatic melanoma, melanoma with untreated brain metastases, and non-melanoma solid tumours. This study is registered with ClinicalTrials.gov, number NCT00880321.
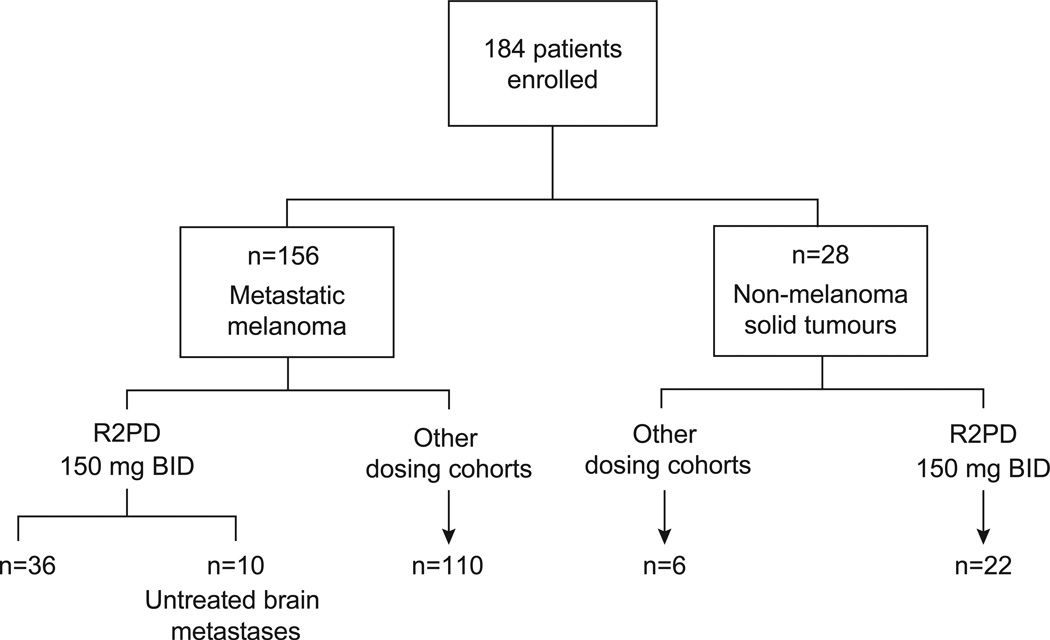
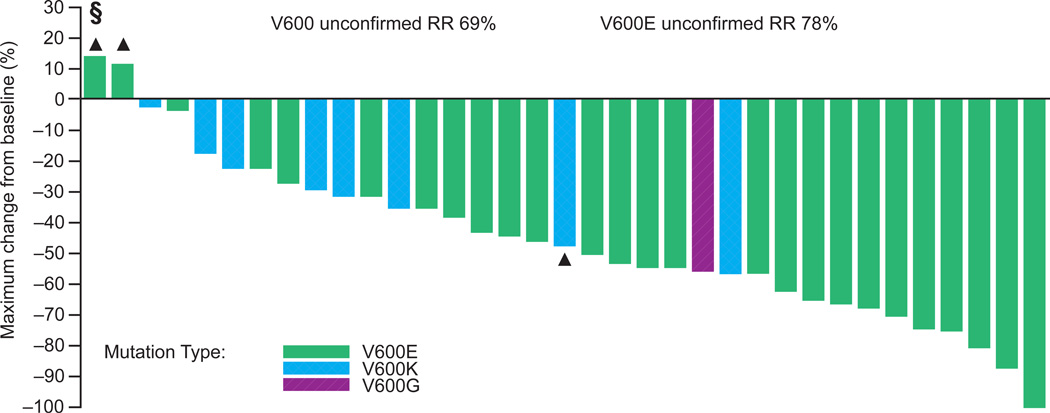
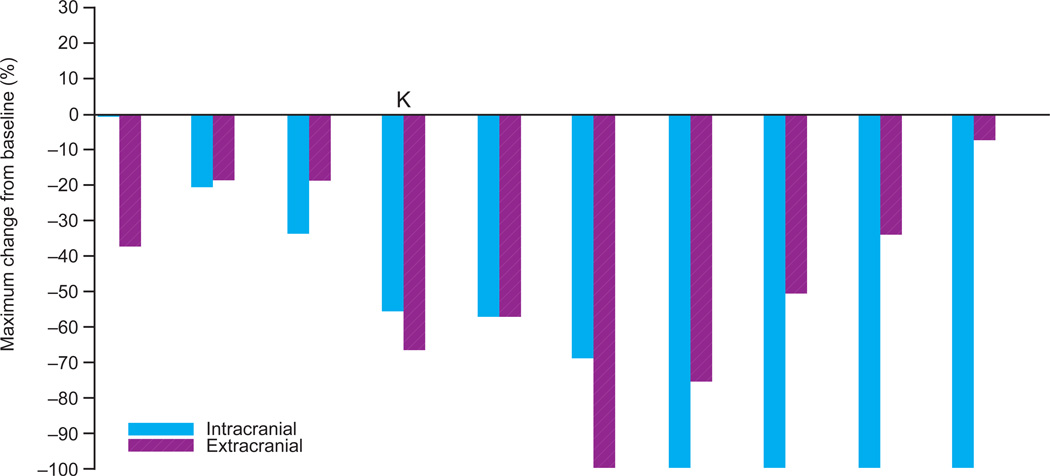
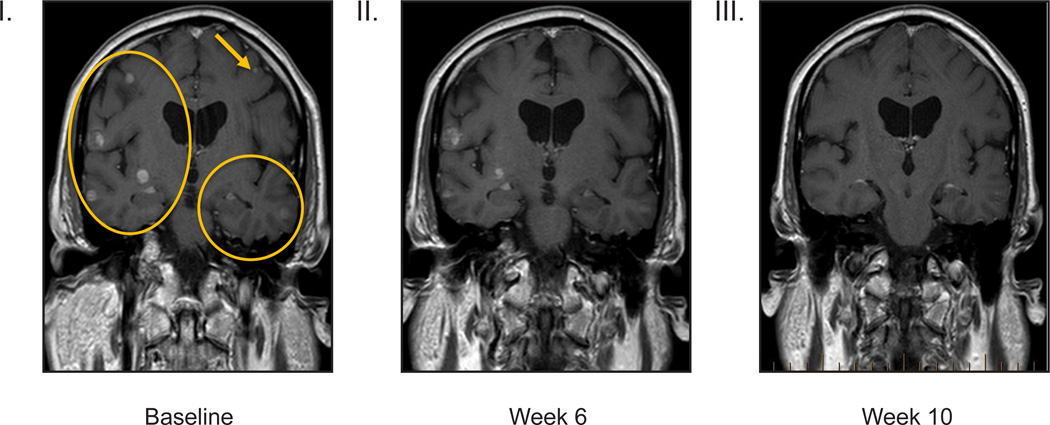
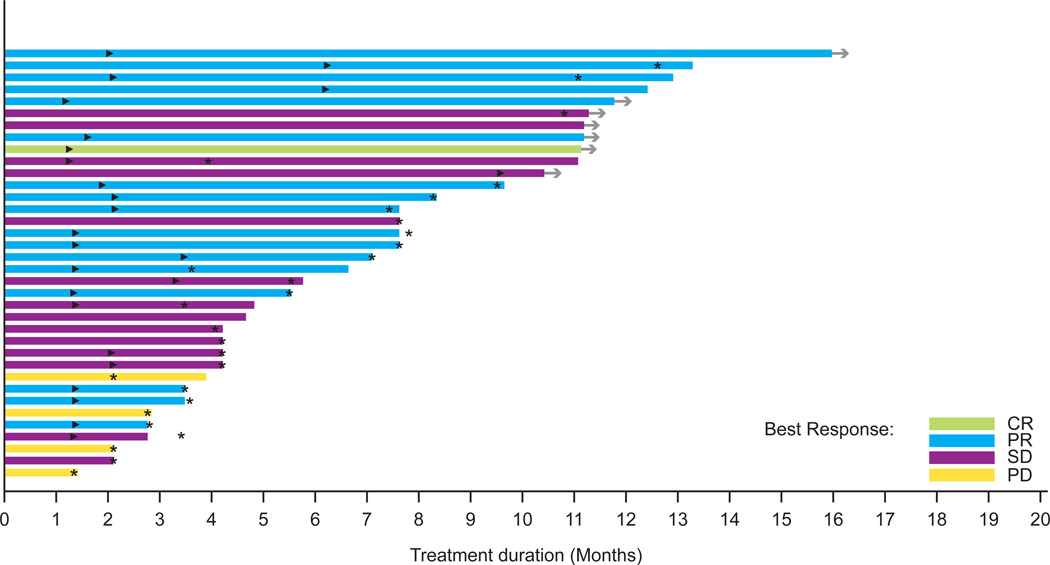
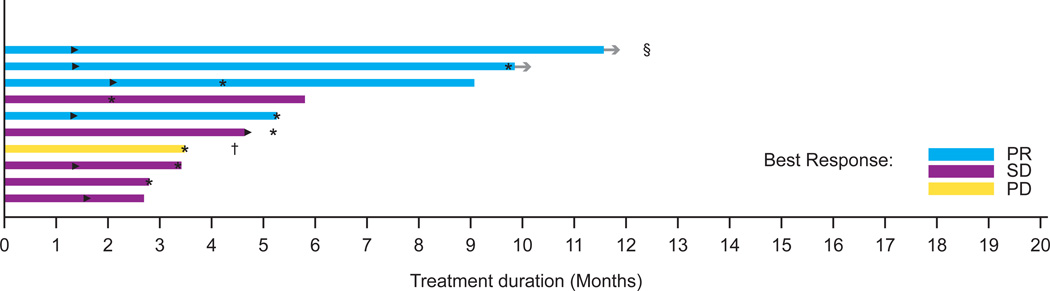
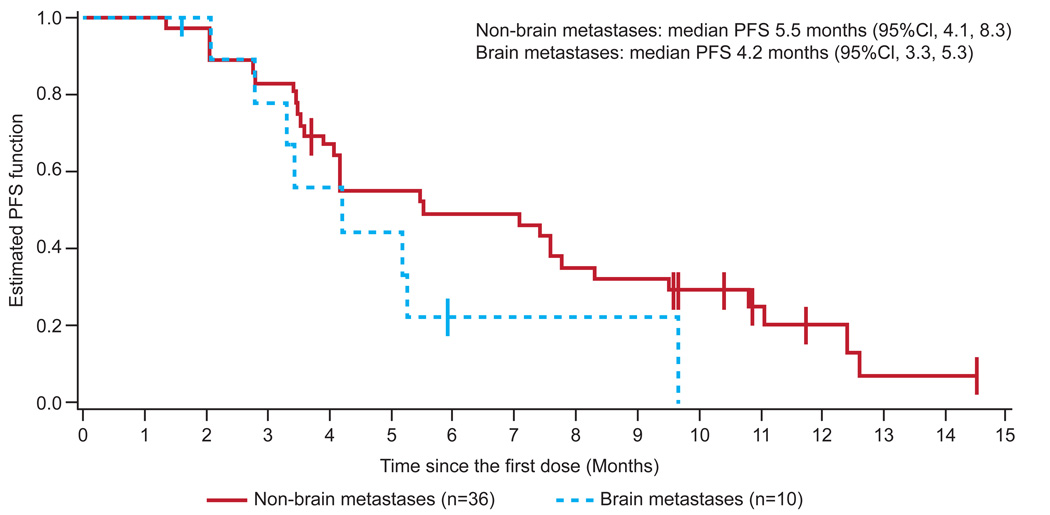
Findings: We enrolled 184 patients, of whom 156 had metastatic melanoma. The most common treatment-related adverse events of grade 2 or worse were cutaneous squamous-cell carcinoma (20 patients, 11%), fatigue (14, 8%), and pyrexia (11, 6%). Dose reductions were necessary in 13 (7%) patients. No deaths or discontinuations resulted from adverse events, and 140 (76%) patients had no treatment-related adverse events worse than grade 2. Doses were increased to 300 mg twice daily, with no maximum tolerated dose recorded. On the basis of safety, pharmacokinetic, and response data, we selected a recommended phase 2 dose of 150 mg twice daily. At the recommended phase 2 dose in 36 patients with Val600 BRAF-mutant melanoma, responses were reported in 25 (69%, 95% CI 51·9-83·7) and confirmed responses in 18 (50%, 32·9-67·1). 21 (78%, 57·7-91·4) of 27 patients with Val600Glu BRAF-mutant melanoma responded and 15 (56%, 35·3-74·5) had a confirmed response. In Val600 BRAF-mutant melanoma, responses were durable, with 17 patients (47%) on treatment for more than 6 months. Responses were recorded in patients with non-Val600Glu BRAF mutations. In patients with melanoma and untreated brain metastases, nine of ten patients had reductions in size of brain lesions. In 28 patients with BRAF-mutant non-melanoma solid tumours, apparent antitumour activity was noted in a gastrointestinal stromal tumour, papillary thyroid cancers, non-small-cell lung cancer, ovarian cancer, and colorectal cancer.
Interpretation: Dabrafenib is safe in patients with solid tumours, and an active inhibitor of Val600-mutant BRAF with responses noted in patients with melanoma, brain metastases, and other solid tumours.
Funding: GlaxoSmithKline.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Gerald Falchook received support for congress attendance from GlaxoSmithKline. The Department of Investigational Cancer Therapeutics, MD Anderson Cancer Center, Houston, Texas received research funds from GlaxoSmithKline on behalf of Gerald Falchook and Razelle Kurzrock. Georgina Long received honoraria from GlaxoSmithKline and Roche, support for congress attendance from GlaxoSmithKline, and payment for lectures from Merck, Sharp & Dohme and Pfizer. The Melanoma Institute Australia received educational grants from Roche. Michael Brown received consultancy fees from GlaxoSmithKline. Omid Hamid received payment for lectures from Genentech and BMS, and The Angeles Clinic received grants for clinical trials from Arqule, BMS, Genentech, and Roche. Drug Development Unit, Sarah Cannon Research Institute, Nashville received consulting fees and support for congress attendance on behalf of Jeffrey Infante, who has no additional personal conflicts of interest. Michael Millward received consultancy fees and the Cancer Council Trials and Sir Charles Gairdner Hospital and University of Western Australia received research funding from GlaxoSmithKline. Samuel Blackman, Martin Curtis, Bo Ma and Danielle Ouellet are employees of GlaxoSmithKline and hold stock options. Peter Lebowitz was an employee of GlaxoSmithKline at the time of the study and holds stock options. Richard Kefford received consultancy fees and support for travel from GlaxoSmithKline, and payment for lectures and board membership from Merck, Sharp & Dohme, Pfizer and Roche. The Melanoma Institute Australia, and University of Sydney, and Westmead Institute for Cancer Research received fees for board membership from Merck, Sharp & Dohme and Roche, and support for congress attendance and research grants from Roche. Tobias Arkenau, Kevin Kim and Anna Pavlick have no conflicts of interest.
Figures
Comment in
-
Extending the reach of BRAF-targeted cancer therapy.Lancet. 2012 May 19;379(9829):1858-9. doi: 10.1016/S0140-6736(12)60610-2. Lancet. 2012. PMID: 22608322 No abstract available.
-
Clinical trials: New options for melanoma?Nat Rev Clin Oncol. 2012 May 29;9(7):368. doi: 10.1038/nrclinonc.2012.95. Nat Rev Clin Oncol. 2012. PMID: 22641362 No abstract available.
References
-
- Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–954. - PubMed
-
- Catalogue of Somatic Mutations in Cancer (COSMIC) website Wellcome Trust Sanger Institute. [Accessed August 2011];2011 at http://www.sanger.ac.uk/genetics/CGP/cosmic/
-
- Roth AD, Tejpar S, Delorenzi M, et al. Prognostic role of KRAS and BRAF in stage II and III resected colon cancer: results of the translational study on the PETACC-3, EORTC 40993, SAKK 60-00 trial. J Clin Oncol. 2010;28:466–474. - PubMed
-
- Elisei R, Ugolini C, Viola D, et al. BRAFV600E Mutation and Outcome of Patients with Papillary Thyroid Carcinoma: A 15-Year Median Follow-Up Study. J Clin Endocrinol Metab. 2008;93:3943–3949. - PubMed
-
- Long GV, Menzies AM, Nagrial AM, et al. Prognostic and Clinicopathologic Associations of Oncogenic BRAF in Metastatic Melanoma. J Clin Oncol. 2011;29:1239–1246. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
