

Cannulation strategy for aortic arch reconstruction using deep hypothermic circulatory arrest
- PMID: 22608717
- PMCID: PMC3631598
- DOI: 10.1016/j.athoracsur.2012.03.053
Cannulation strategy for aortic arch reconstruction using deep hypothermic circulatory arrest
Abstract
Background: Aortic arch reconstruction in neonates is commonly performed using deep hypothermic circulatory arrest. However, concerns have arisen regarding potential adverse neurologic outcomes from this complex procedure, raising questions about the best arterial cannulation approach for cerebral perfusion and effective systemic hypothermia. In this study, we use computational fluid dynamics to investigate the effect of different cannulation strategies in neonates.
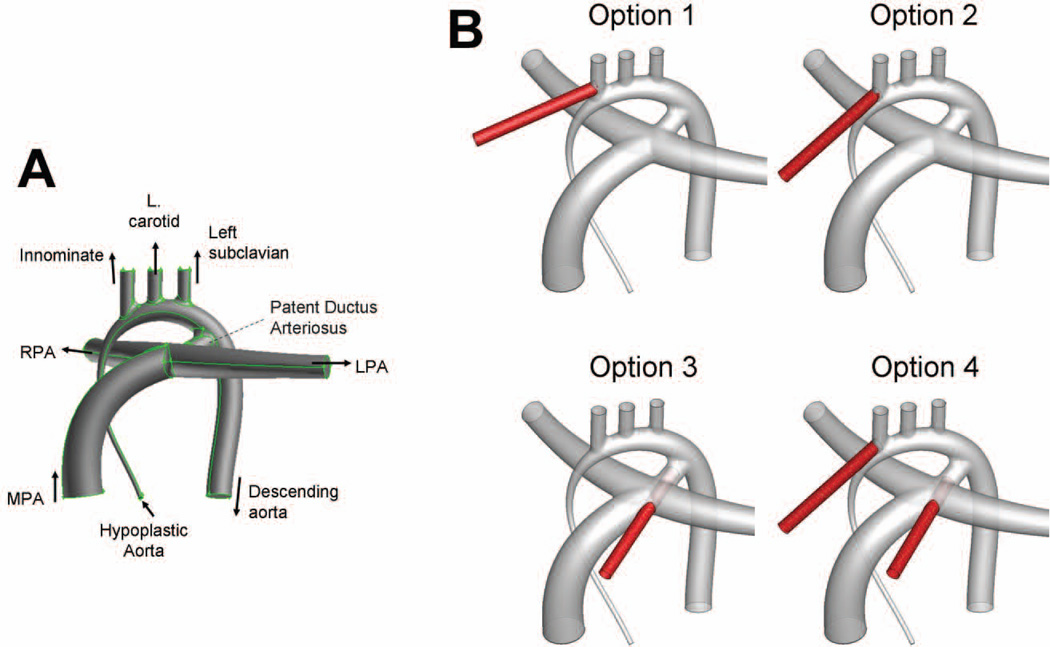
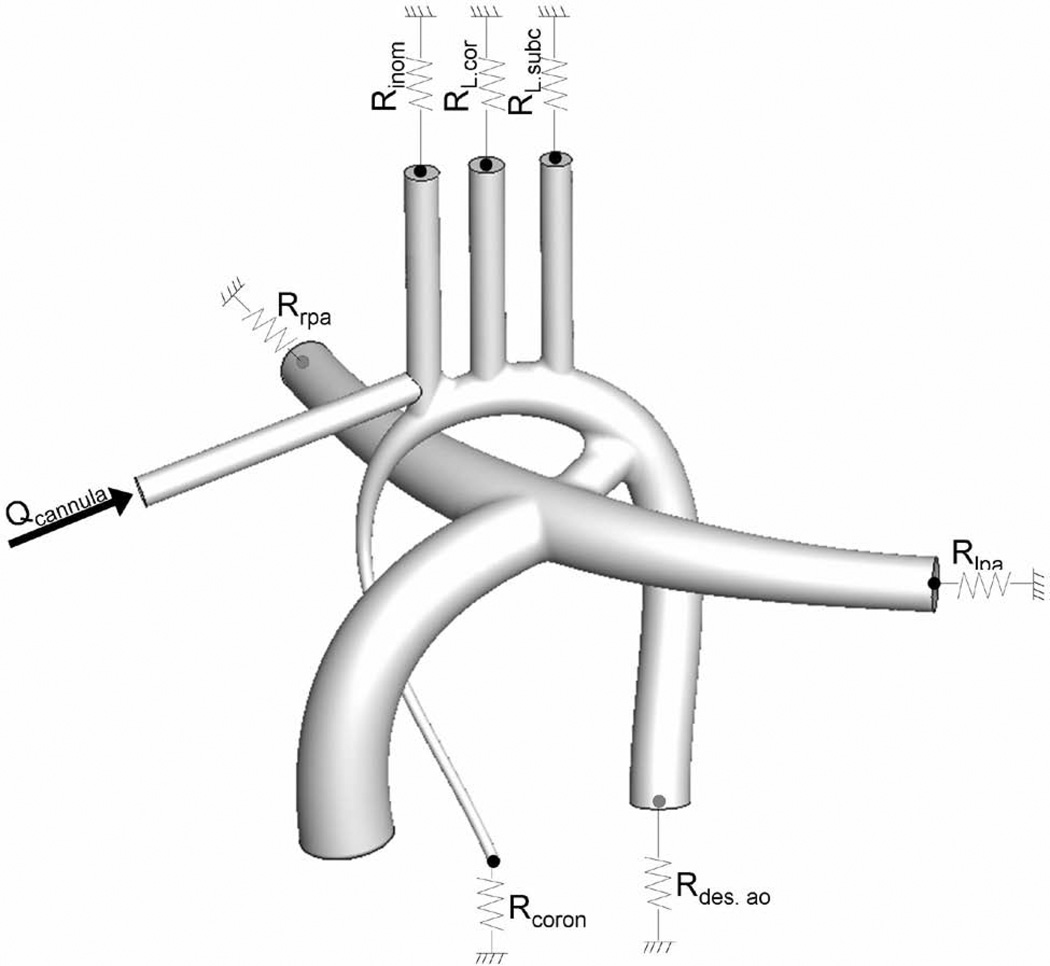
Methods: We used a realistic template of a hypoplastic neonatal aorta as the base geometry to investigate four cannulation options: (1) right innominate artery, (2) innominate root, (3) patent ductus arteriosus (PDA), or (4) innominate root and PDA. Performance was evaluated according to the numerically predicted cerebral and systemic flow distributions compared with physiologic perfusion under neonatal conditions.
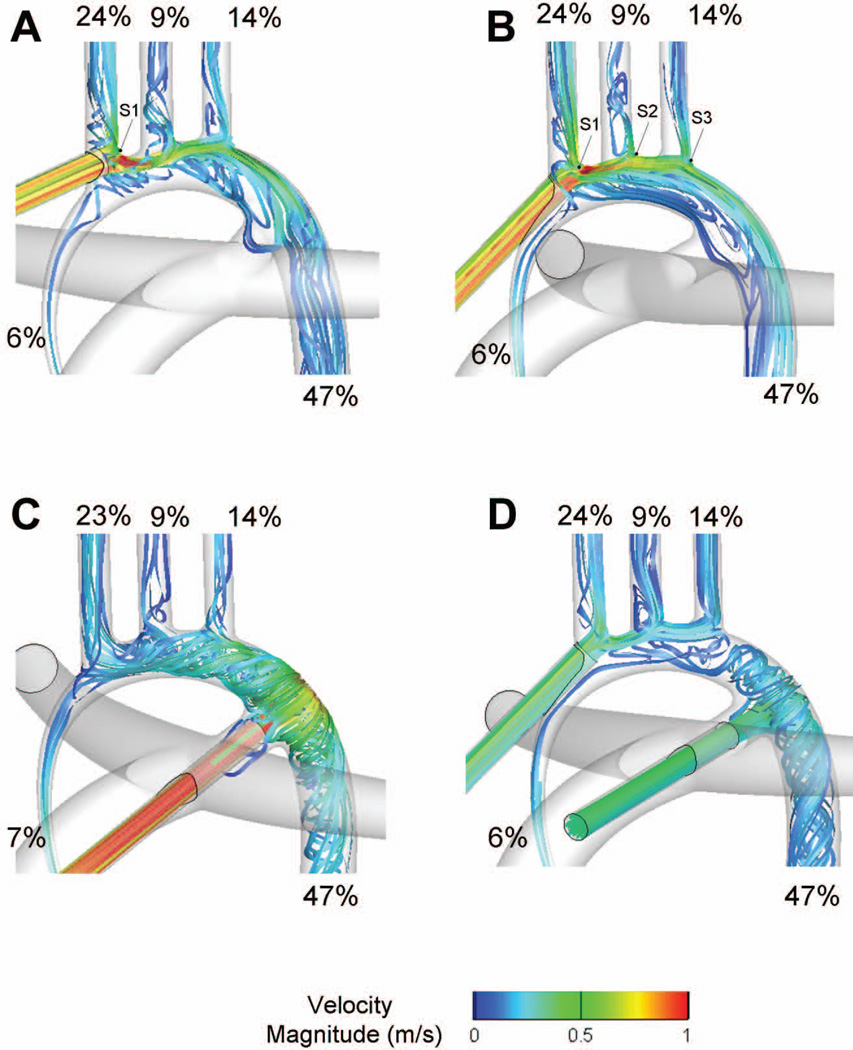
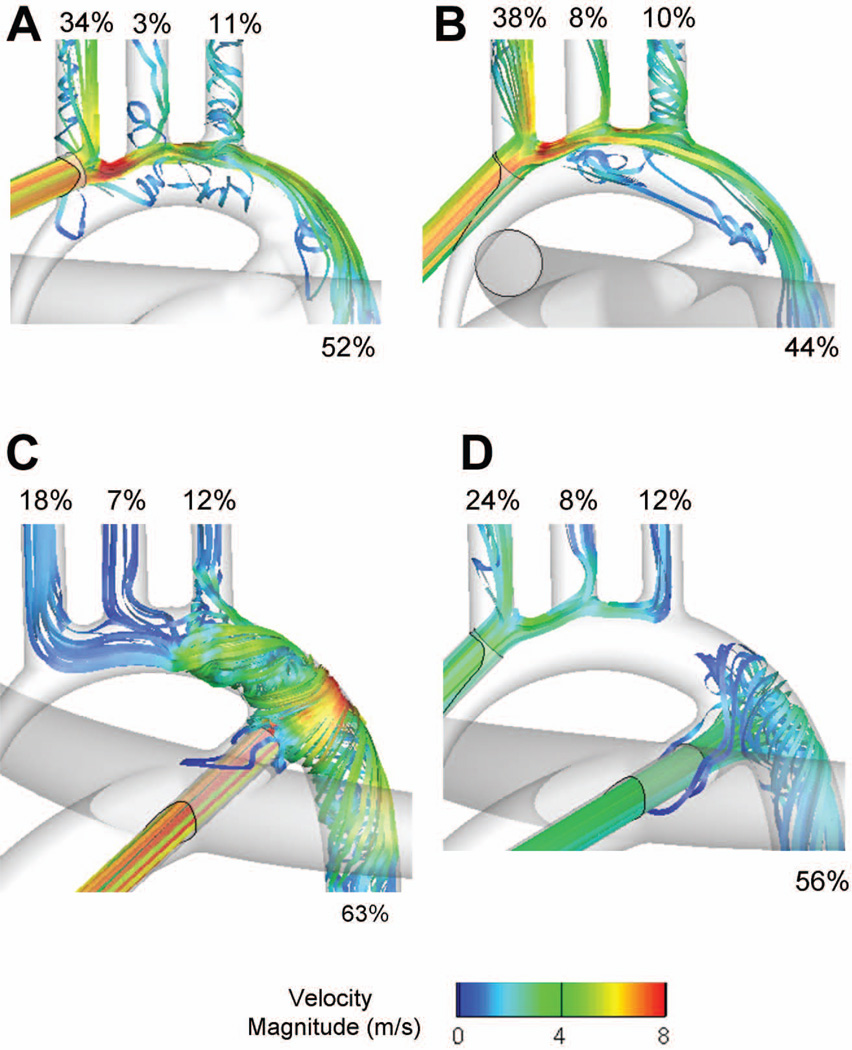
Results: The four cannulation strategies were associated with different local hemodynamics; however, this did not translate into any significant effect on the measured flow distributions. The largest difference only represented 0.8% of the cardiac output and was measured in the innominate artery, which received 23.2% of the cardiac output in option 3 vs 24% in option 4. Pulmonary artery snaring benefited all systemic vessels uniformly.
Conclusions: Because of the very high vascular resistances in neonates, downstream vascular resistances dictated flow distribution to the different vascular beds rather than the cannulation strategy, allowing the surgical team to choose their method of preference. However, patients with aortic coarctation warrant further investigation and will most likely benefit from a 2-cannulae approach (option 4).
Copyright © 2012 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited commentary.Ann Thorac Surg. 2012 Aug;94(2):621. doi: 10.1016/j.athoracsur.2012.04.015. Ann Thorac Surg. 2012. PMID: 22818308 No abstract available.
Similar articles
-
Clinical Assessment of Perfusion Techniques During Surgical Repair of Coarctation of Aorta With Aortic Arch Hypoplasia in Neonates: A Pilot Prospective Randomized Study.Semin Thorac Cardiovasc Surg. 2020 Winter;32(4):860-871. doi: 10.1053/j.semtcvs.2020.04.015. Epub 2020 May 22. Semin Thorac Cardiovasc Surg. 2020. PMID: 32446921 Clinical Trial.
-
Neonatal aortic arch reconstruction avoiding circulatory arrest and direct arch vessel cannulation.Ann Thorac Surg. 2001 Nov;72(5):1615-20. doi: 10.1016/s0003-4975(01)03063-6. Ann Thorac Surg. 2001. PMID: 11722054
-
Newborn aortic arch reconstruction with descending aortic cannulation improves postoperative renal function.Ann Thorac Surg. 2013 Nov;96(5):1721-6; discussion 1726. doi: 10.1016/j.athoracsur.2013.06.033. Epub 2013 Aug 30. Ann Thorac Surg. 2013. PMID: 23998412
-
Is moderate hypothermic circulatory arrest with selective antegrade cerebral perfusion superior to deep hypothermic circulatory arrest in elective aortic arch surgery?Interact Cardiovasc Thorac Surg. 2016 Sep;23(3):462-8. doi: 10.1093/icvts/ivw124. Epub 2016 May 21. Interact Cardiovasc Thorac Surg. 2016. PMID: 27209532 Review.
-
Supplemental Perfusion Techniques for Aortic Arch Reconstruction, With Emphasis on Direct Cannulation of the Descending Aorta.Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2019;22:14-20. doi: 10.1053/j.pcsu.2019.02.010. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2019. PMID: 31027558 Review.
Cited by
-
Cervical Cannulation for Surgical Repair of Congenital Cardiac Defects in Infants and Small Children.Braz J Cardiovasc Surg. 2017 Mar-Apr;32(2):111-117. doi: 10.21470/1678-9741-2016-0083. Braz J Cardiovasc Surg. 2017. PMID: 28492792 Free PMC article.
-
Use of carotid artery cannulation during redo sternotomy in congenital cardiac surgery: a single-centre experience.Interact Cardiovasc Thorac Surg. 2021 Jun 28;33(1):119-123. doi: 10.1093/icvts/ivab060. Interact Cardiovasc Thorac Surg. 2021. PMID: 33704457 Free PMC article.
-
Is Decellularized Porcine Small Intestine Sub-mucosa Patch Suitable for Aortic Arch Repair?Front Pediatr. 2018 May 30;6:149. doi: 10.3389/fped.2018.00149. eCollection 2018. Front Pediatr. 2018. PMID: 29900163 Free PMC article.
-
Development of idealized human aortic models for in vitro and in silico hemodynamic studies.Front Cardiovasc Med. 2024 Aug 5;11:1358601. doi: 10.3389/fcvm.2024.1358601. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39161662 Free PMC article.
-
Tetralogy of Fallot Surgical Repair: Shunt Configurations, Ductus Arteriosus and the Circle of Willis.Cardiovasc Eng Technol. 2017 Jun;8(2):107-119. doi: 10.1007/s13239-017-0302-5. Epub 2017 Apr 5. Cardiovasc Eng Technol. 2017. PMID: 28382440 Free PMC article.
References
-
- Wypij D, Newburger JW, Rappaport LA, duPlessis AJ, Jonas RA, Wernovsky G, Lin M, Bellinger DC. The effect of duration of deep hypothermic circulatory arrest in infant heart surgery on late neurodevelopment: The Boston Circulatory Arrest Trial. Journal of Thoracic and Cardiovascular Surgery. 2003;126(5):1397–1403. - PubMed
-
- Okita Y, Ando M, Minatoya K, Kitamura S, Takamoto S, Nakajima N. Predictive factors for mortality and cerebral complications in arteriosclerotic aneurysm of the aortic arch. Ann Thorac Surg. 1999;67(1):72–78. - PubMed
-
- Tchervenkov CI, Korkola SJ, Shum-Tim D. Surgical technique to avoid circulatory arrest and direct arch vessel cannulation during neonatal aortic arch reconstruction. Eur J Cardiothorac Surg. 2001;19(5):708–710. - PubMed
-
- Gerdes A, Joubert-Hubner E, Esders K, Sievers HH. Hydrodynamics of aortic arch vessels during perfusion through the right subclavian artery. Ann Thorac Surg. 2000;69(5):1425–1430. - PubMed
-
- Poirier NC, Drummond-Webb JJ, Hisamochi K, Imamura M, Harrison AM, Mee RB. Modified Norwood procedure with a high-flow cardiopulmonary bypass strategy results in low mortality without late arch obstruction. J Thorac Cardiovasc Surg. 2000;120(5):875–884. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
