

Maternal BMI, glucose tolerance, and adverse pregnancy outcomes
- PMID: 22609018
- PMCID: PMC3482614
- DOI: 10.1016/j.ajog.2012.04.035
Maternal BMI, glucose tolerance, and adverse pregnancy outcomes
Abstract
Objective: The purpose of this study was to estimate the association of pregravid body mass index (BMI), independent of 3-hour oral glucose tolerance test (OGTT) results, with pregnancy outcome.
Study design: In this secondary analysis of a cohort of women with untreated mild gestational glucose intolerance, which was defined as a 50-g glucose loading test between 135 and 199 mg/dL and fasting glucose level of <95 mg/dL, we modeled the association between pregravid BMI, OGTT results, and both pregnancy complications and neonatal adiposity.
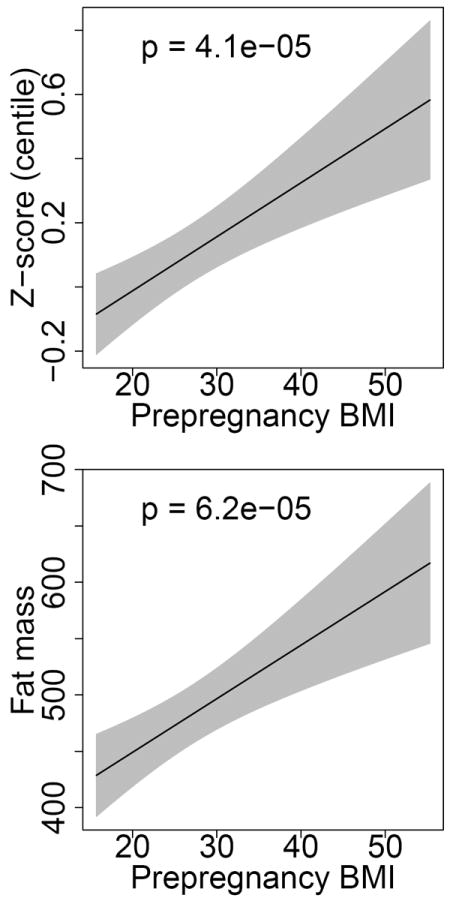
Results: Among 1250 participants, both pregravid BMI and glucose at hour 3 of the OGTT were associated with increased risk of gestational hypertension. Maternal pregravid BMI also was associated positively with large-for-gestational-age infants; both maternal BMI and fasting glucose were associated with birthweight z-score and neonatal fat mass.
Conclusion: Among women with untreated mild gestational glucose intolerance, pregravid BMI is associated with increased gestational hypertension, birthweight, and neonatal fat mass, independent of OGTT values.
Copyright © 2012 Mosby, Inc. All rights reserved.
Conflict of interest statement
Disclosure: None of the authors have a conflict of interest.
Figures

References
-
- Callaway LK, Prins JB, Chang AM, McIntyre HD. The prevalence and impact of overweight and obesity in an Australian obstetric population. Med J Aust. 2006;184:56–9. - PubMed
-
- Driul L, Cacciaguerra G, Citossi A, Martina MD, Peressini L, Marchesoni D. Prepregnancy body mass index and adverse pregnancy outcomes. Arch Gynecol Obstet. 2008;278:23–6. - PubMed
-
- Khashan AS, Kenny LC. The effects of maternal body mass index on pregnancy outcome. Eur J Epidemiol. 2009;24:697–705. - PubMed
-
- Sebire NJ, Jolly M, Harris JP, et al. Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. Int J Obes Relat Metab Disord. 2001;25:1175–82. - PubMed
Publication types
MeSH terms
Grants and funding
- HD36801/HD/NICHD NIH HHS/United States
- U10 HD040544/HD/NICHD NIH HHS/United States
- U10 HD040485/HD/NICHD NIH HHS/United States
- UL1-RR024989/RR/NCRR NIH HHS/United States
- HD40485/HD/NICHD NIH HHS/United States
- HD40560/HD/NICHD NIH HHS/United States
- 5K12HD050113-04/HD/NICHD NIH HHS/United States
- U10 HD040512/HD/NICHD NIH HHS/United States
- U01 HD036801/HD/NICHD NIH HHS/United States
- U10 HD053118/HD/NICHD NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- U10 HD040500/HD/NICHD NIH HHS/United States
- M01-RR00034/RR/NCRR NIH HHS/United States
- UG1 HD027869/HD/NICHD NIH HHS/United States
- M01 RR000034/RR/NCRR NIH HHS/United States
- UL1-RR025764/RR/NCRR NIH HHS/United States
- UL1 RR025764/RR/NCRR NIH HHS/United States
- UG1 HD034116/HD/NICHD NIH HHS/United States
- HD27869/HD/NICHD NIH HHS/United States
- HD34136/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- U10 HD034136/HD/NICHD NIH HHS/United States
- K12 HD050113/HD/NICHD NIH HHS/United States
- HD53118/HD/NICHD NIH HHS/United States
- UG1 HD053097/HD/NICHD NIH HHS/United States
- HD27860/HD/NICHD NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- HD40512/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- HD40545/HD/NICHD NIH HHS/United States
- U10 HD034116/HD/NICHD NIH HHS/United States
- HD21410/HD/NICHD NIH HHS/United States
- U10 HD027869/HD/NICHD NIH HHS/United States
- U10 HD027917/HD/NICHD NIH HHS/United States
- HD34116/HD/NICHD NIH HHS/United States
- U10 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- U10 HD027860/HD/NICHD NIH HHS/United States
- HD40500/HD/NICHD NIH HHS/United States
- C06 RR011234/RR/NCRR NIH HHS/United States
- U10 HD040560/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- U10 HD053097/HD/NICHD NIH HHS/United States
- HD34208/HD/NICHD NIH HHS/United States
- HD27915/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- M01-RR00080/RR/NCRR NIH HHS/United States
- HD27917/HD/NICHD NIH HHS/United States
- U10 HD021410/HD/NICHD NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- HD53097/HD/NICHD NIH HHS/United States
- U10 HD040545/HD/NICHD NIH HHS/United States
- HD40544/HD/NICHD NIH HHS/United States
