

Plasma angiopoietin-2 in clinical acute lung injury: prognostic and pathogenetic significance
- PMID: 22610178
- PMCID: PMC3601049
- DOI: 10.1097/CCM.0b013e3182451c87
Plasma angiopoietin-2 in clinical acute lung injury: prognostic and pathogenetic significance
Abstract
Background: Angiopoietin-2 is a proinflammatory mediator of endothelial injury in animal models, and increased plasma angiopoietin-2 levels are associated with poor outcomes in patients with sepsis-associated acute lung injury. Whether angiopoietin-2 levels are modified by treatment strategies in patients with acute lung injury is unknown.
Objectives: To determine whether plasma angiopoietin-2 levels are associated with clinical outcomes and affected by fluid management strategy in a broad cohort of patients with acute lung injury.
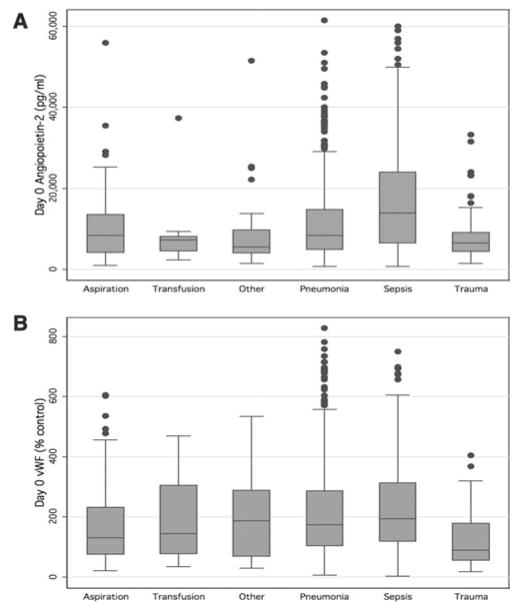
Design, setting, and participants: Plasma levels of angiopoietin-2 and von Willebrand factor (a traditional marker of endothelial injury) were measured in 931 subjects with acute lung injury enrolled in a randomized trial of fluid liberal vs. fluid conservative management.
Measurements and main results: The presence of infection (sepsis or pneumonia) as the primary acute lung injury risk factor significantly modified the relationship between baseline angiopoietin-2 levels and mortality (p = .01 for interaction). In noninfection-related acute lung injury, higher baseline angiopoietin-2 levels were strongly associated with increased mortality (odds ratio, 2.43 per 1-log increase in angiopoietin-2; 95% confidence interval, 1.57-3.75; p < .001). In infection-related acute lung injury, baseline angiopoietin-2 levels were similarly elevated in survivors and nonsurvivors; however, patients whose plasma angiopoietin-2 levels increased from day 0 to day 3 had more than double the odds of death compared with patients whose angiopoietin-2 levels declined over the same period of time (odds ratio, 2.29; 95% confidence interval, 1.54-3.43; p < .001). Fluid-conservative therapy led to a 15% greater decline in angiopoietin-2 levels from day 0 to day 3 (95% confidence interval, 4.6-24.8%; p = .006) compared with fluid-liberal therapy in patients with infection-related acute lung injury. In contrast, plasma levels of von Willebrand factor were significantly associated with mortality in both infection-related and noninfection-related acute lung injury and were not affected by fluid therapy.
Conclusions: Unlike von Willebrand factor, plasma angiopoietin-2 has differential prognostic value for mortality depending on the presence or absence of infection as an acute lung injury risk factor. Fluid conservative therapy preferentially lowers plasma angiopoietin-2 levels over time and thus may be beneficial in part by decreasing endothelial inflammation.
Conflict of interest statement
The remaining authors have not disclosed any potential conflicts of interest.
Figures

Comment in
-
von Willebrand factor and angiopoietin-2: toward an acute lung injury endothelial endophenotype?Crit Care Med. 2012 Jun;40(6):1966-7. doi: 10.1097/CCM.0b013e31824c8fad. Crit Care Med. 2012. PMID: 22610202 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
