

Basal cell carcinoma of the head and neck region in ethnic chinese
- PMID: 22611492
- PMCID: PMC3265281
- DOI: 10.1155/2011/890908
Basal cell carcinoma of the head and neck region in ethnic chinese
Abstract
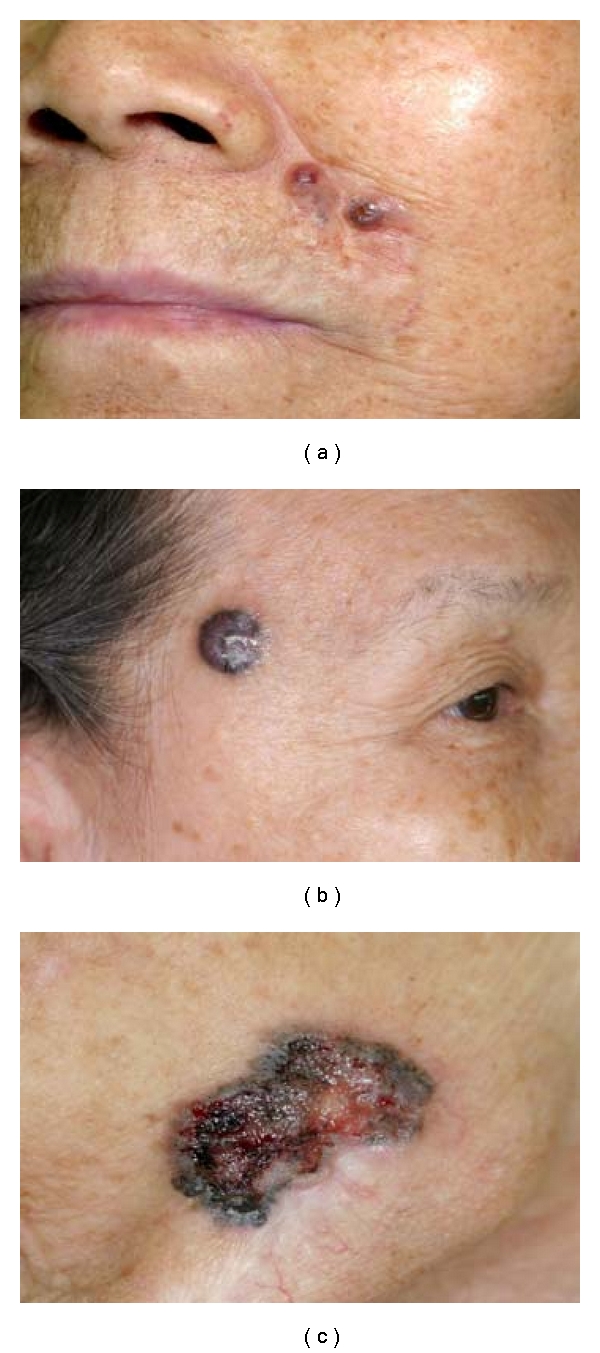
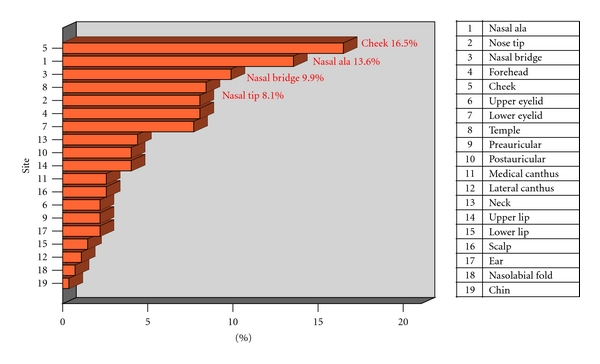
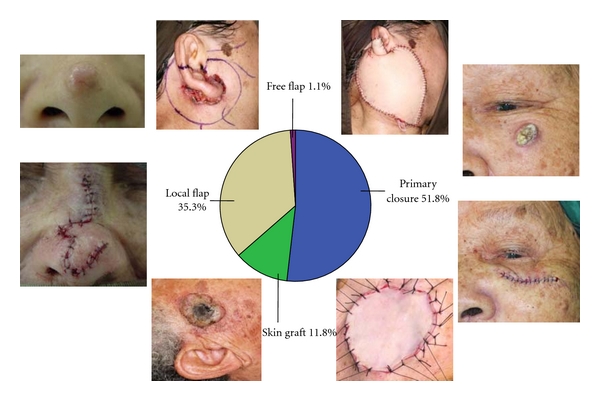
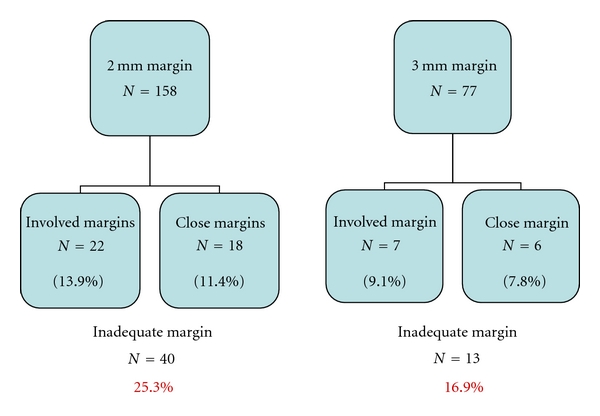
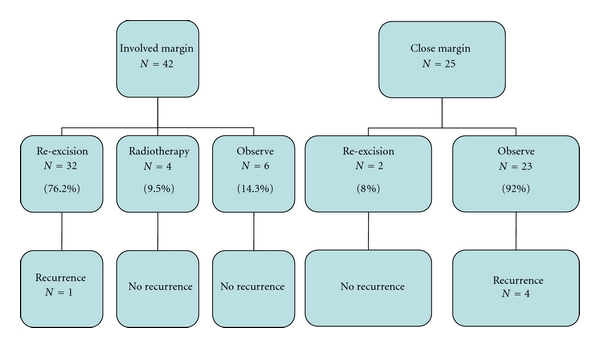
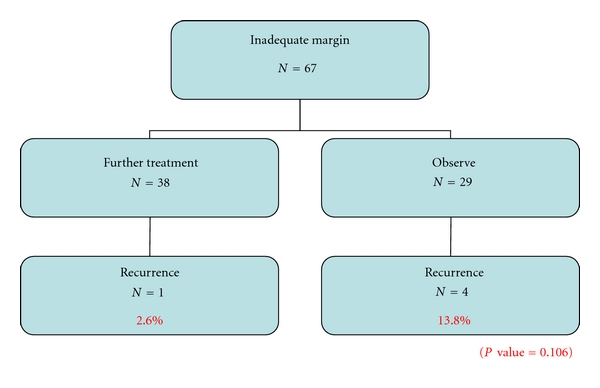
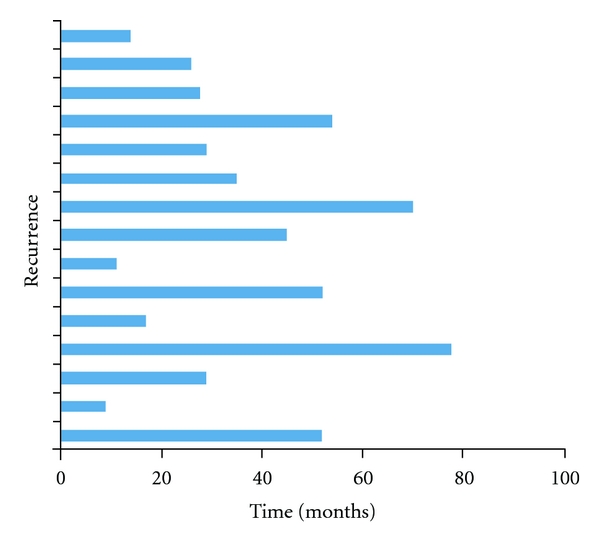
Objectives. This study aims to report our experience in the management of HNBCC in ethnic Chinese over a 10-year period. Methods. A retrospective review of all ethnic Chinese patients with HNBCC treated in a tertiary centre from 1999 to 2009. Results. From 1999 to 2009, 225 patients underwent surgical excision for HNBCC. Majority were elderly female patients. Commonest presentation was a pigmented (76.2%) ulcer (64.8%) over the nose (31.6%). Median skin margin taken on tumour excision was 2.0 mm; primary skin closure was achieved in 51.8%. Postresection skin margin was clear in 75.4%. Of those with inadequate skin margins, 56.7% opted for further treatment, 43.4% for observation. Recurrence rates were 2.6% and 13.8%, respectively (P = 0.106). Overall recurrence rate was 5.5%. Conclusions. HNBCC commonly presented as pigmented ulcers over the nose of elderly female patients in our locality. Adequate tumour excision ± reconstruction offered the best chance of cure. Reexcision of those with inadequate skin margins improved local tumour control.
Figures
Similar articles
-
Surgical management of melanoma-in-situ using a staged marginal and central excision technique.Ann Surg Oncol. 2009 Jun;16(6):1526-36. doi: 10.1245/s10434-008-0239-x. Epub 2008 Dec 3. Ann Surg Oncol. 2009. PMID: 19050971
-
Multimodality management of high-risk head and neck basal cell carcinoma requiring free-flap reconstruction.Otolaryngol Head Neck Surg. 2015 May;152(5):868-73. doi: 10.1177/0194599815575720. Epub 2015 Mar 24. Otolaryngol Head Neck Surg. 2015. PMID: 25805638
-
Clinical and Financial Implications of Positive Margins After Nonmelanoma Skin Cancer Resection: A Longitudinal Evaluation.Ann Plast Surg. 2021 Jul 1;87(1):80-84. doi: 10.1097/SAP.0000000000002566. Ann Plast Surg. 2021. PMID: 33009148
-
Basal cell carcinoma of the head and neck region--a five-year study (1984-88).Ann Acad Med Singap. 1990 Mar;19(2):182-5. Ann Acad Med Singap. 1990. PMID: 2346293
-
Tumour-free margins in vulvar squamous cell carcinoma: Does distance really matter?Eur J Cancer. 2016 Sep;65:139-49. doi: 10.1016/j.ejca.2016.07.006. Epub 2016 Aug 3. Eur J Cancer. 2016. PMID: 27497345 Review.
Cited by
-
A study of Basal cell carcinoma in South asians for risk factor and clinicopathological characterization: a hospital based study.J Skin Cancer. 2014;2014:173582. doi: 10.1155/2014/173582. Epub 2014 Nov 3. J Skin Cancer. 2014. PMID: 25530883 Free PMC article.
-
Head and neck cutaneous basal cell carcinoma: a retrospective analysis of tumour features, surgical margins and recurrences.Eur Arch Otorhinolaryngol. 2025 Jun;282(6):3183-3191. doi: 10.1007/s00405-025-09216-z. Epub 2025 Feb 20. Eur Arch Otorhinolaryngol. 2025. PMID: 39979627 Free PMC article.
-
Basal Cell Carcinoma Surgery in general practice: Is there a role for the local General Practitioner?Malays Fam Physician. 2020 Nov 10;15(3):10-21. eCollection 2020. Malays Fam Physician. 2020. PMID: 33329859 Free PMC article. Review.
-
New Forehead, New Confidence: Flap Advancement Post-cancer Excision.Cureus. 2025 Mar 30;17(3):e81458. doi: 10.7759/cureus.81458. eCollection 2025 Mar. Cureus. 2025. PMID: 40303544 Free PMC article.
-
Surgical treatment of basal cell carcinoma: an algorithm based on the literature.An Bras Dermatol. 2015 May-Jun;90(3):377-83. doi: 10.1590/abd1806-4841.20153304. Epub 2015 Jun 1. An Bras Dermatol. 2015. PMID: 26131869 Free PMC article. Review.
References
-
- American Cancer Society. Detailed guide: skin cancer–basal and squamous cell
-
- Cancer Research UK. CancerStats Key facts on skin cancer. How common is skin cancer? http://info.cancerresearchuk.org/cancerstats/types/skin/#incidence.
-
- Katalinic A, Kunze U, Schäfer T. Epidemiology of cutaneous melanoma and non-melanoma skin cancer in Schleswig-Holstein, Germany: incidence, clinical subtypes, tumour stages and localization (epidemiology of skin cancer) British Journal of Dermatology. 2003;149(6):1200–1206. - PubMed
-
- Staples MP, Elwood M, Burton RC, Williams JL, Marks R, Giles GG. Non-melanoma skin cancer in Australia: the 2002 national survey and trends since 1985. Medical Journal of Australia. 2006;184(1):6–10. - PubMed
-
- Hayes RC, Leonfellner S, Pilgrim W, Liu J, Keeling DN. Incidence of nonmelanoma skin cancer in New Brunswick, Canada, 1992 to 2001. Journal of Cutaneous Medicine and Surgery. 2007;11(2):45–52. - PubMed
LinkOut - more resources
Full Text Sources
