

Nighttime intensivist staffing and mortality among critically ill patients
- PMID: 22612639
- PMCID: PMC3979289
- DOI: 10.1056/NEJMsa1201918
Nighttime intensivist staffing and mortality among critically ill patients
Erratum in
- N Engl J Med. 2012 Aug 30;367(9):881
Abstract
Background: Hospitals are increasingly adopting 24-hour intensivist physician staffing as a strategy to improve intensive care unit (ICU) outcomes. However, the degree to which nighttime intensivists are associated with improvements in the quality of ICU care is unknown.
Methods: We conducted a retrospective cohort study involving ICUs that participated in the Acute Physiology and Chronic Health Evaluation (APACHE) clinical information system from 2009 through 2010, linking a survey of ICU staffing practices with patient-level outcomes data from adult ICU admissions. Multivariate models were used to assess the relationship between nighttime intensivist staffing and in-hospital mortality among ICU patients, with adjustment for daytime intensivist staffing, severity of illness, and case mix. We conducted a confirmatory analysis in a second, population-based cohort of hospitals in Pennsylvania from which less detailed data were available.
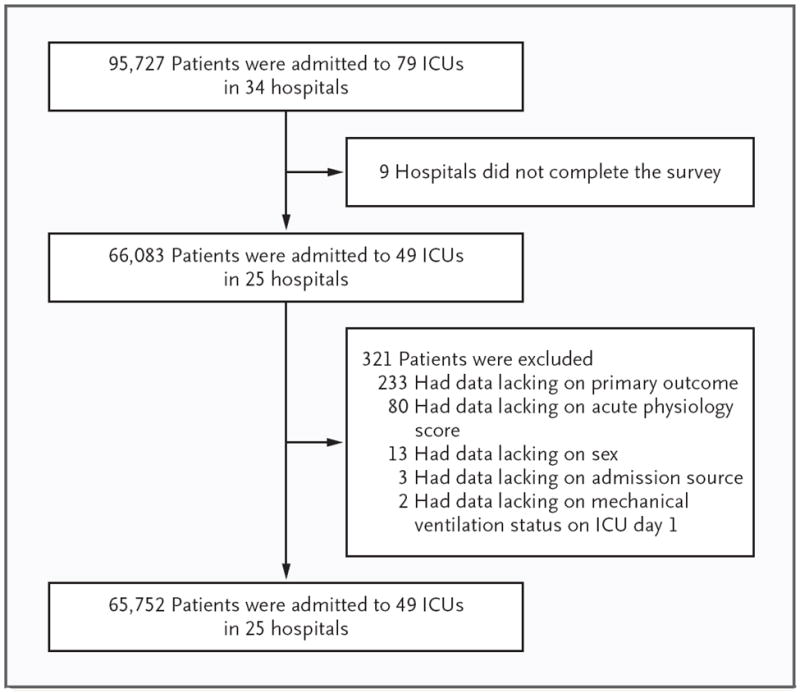
Results: The analysis with the use of the APACHE database included 65,752 patients admitted to 49 ICUs in 25 hospitals. In ICUs with low-intensity daytime staffing, nighttime intensivist staffing was associated with a reduction in risk-adjusted in-hospital mortality (adjusted odds ratio for death, 0.62; P=0.04). Among ICUs with high-intensity daytime staffing, nighttime intensivist staffing conferred no benefit with respect to risk-adjusted in-hospital mortality (odds ratio, 1.08; P=0.78). In the verification cohort, there was a similar relationship among daytime staffing, nighttime staffing, and in-hospital mortality. The interaction between nighttime staffing and daytime staffing was not significant (P=0.18), yet the direction of the findings were similar to those in the APACHE cohort.
Conclusions: The addition of nighttime intensivist staffing to a low-intensity daytime staffing model was associated with reduced mortality. However, a reduction in mortality was not seen in ICUs with high-intensity daytime staffing. (Funded by the National Heart, Lung, and Blood Institute.).
Figures
Comment in
-
Intensive enough?N Engl J Med. 2012 May 31;366(22):2124-5. doi: 10.1056/NEJMe1203772. Epub 2012 May 21. N Engl J Med. 2012. PMID: 22612640 No abstract available.
-
Nighttime intensivist staffing.N Engl J Med. 2012 Sep 6;367(10):971; author reply 972. doi: 10.1056/NEJMc1207796. N Engl J Med. 2012. PMID: 22931273 No abstract available.
-
Nighttime intensivist staffing.N Engl J Med. 2012 Sep 6;367(10):971; author reply 972. doi: 10.1056/NEJMc1207796. N Engl J Med. 2012. PMID: 22931274 No abstract available.
-
Nighttime intensivist staffing.N Engl J Med. 2012 Sep 6;367(10):971-2; author reply 972. doi: 10.1056/NEJMc1207796. N Engl J Med. 2012. PMID: 22931275 No abstract available.
References
-
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA. 2002;288:2151–62. - PubMed
-
- Haupt MT, Bekes CE, Brilli RJ, et al. Guidelines on critical care services and personnel: recommendations based on a system of categorization of three levels of care. Crit Care Med. 2003;31:2677–83. - PubMed
-
- Burnham EL, Moss M, Geraci MW. The case for 24/7 in-house intensivist coverage. Am J Respir Crit Care Med. 2010;181:1159–60. - PubMed
-
- Cartin-Ceba R, Bajwa EK. 24-Hour on-site intensivist in the intensive care unit: yes. Am J Respir Crit Care Med. 2010;181:1279–80. - PubMed
-
- Jones SF, Gaggar A. Is there a doctor in the house? The downside of 24/7 attending coverage in academic intensive care units. Am J Respir Crit Care Med. 2010;181:1280–1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources