

Elevated plasma levels of heparin-binding protein in intensive care unit patients with severe sepsis and septic shock
- PMID: 22613179
- PMCID: PMC3580636
- DOI: 10.1186/cc11353
Elevated plasma levels of heparin-binding protein in intensive care unit patients with severe sepsis and septic shock
Abstract
Introduction: Rapid detection of, and optimized treatment for, severe sepsis and septic shock is crucial for successful outcome. Heparin-binding protein (HBP), a potent inducer of increased vascular permeability, is a potentially useful biomarker for predicting outcome in patients with severe infections. Our aim was to study the systemic release and dynamics of HBP in the plasma of patients with severe sepsis and septic shock in the ICU.
Methods: A prospective study was conducted of two patient cohorts treated in the ICU at Karolinska University Hospital Huddinge in Sweden. A total of 179 patients was included, of whom 151 had sepsis (126 with septic shock and 25 patients with severe sepsis) and 28 a non-septic critical condition. Blood samples were collected at five time points during six days after admission.
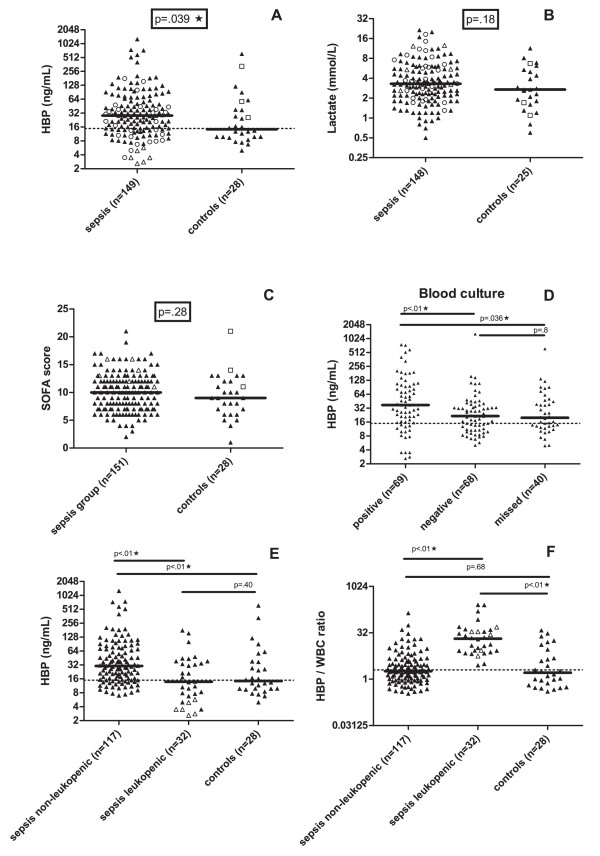
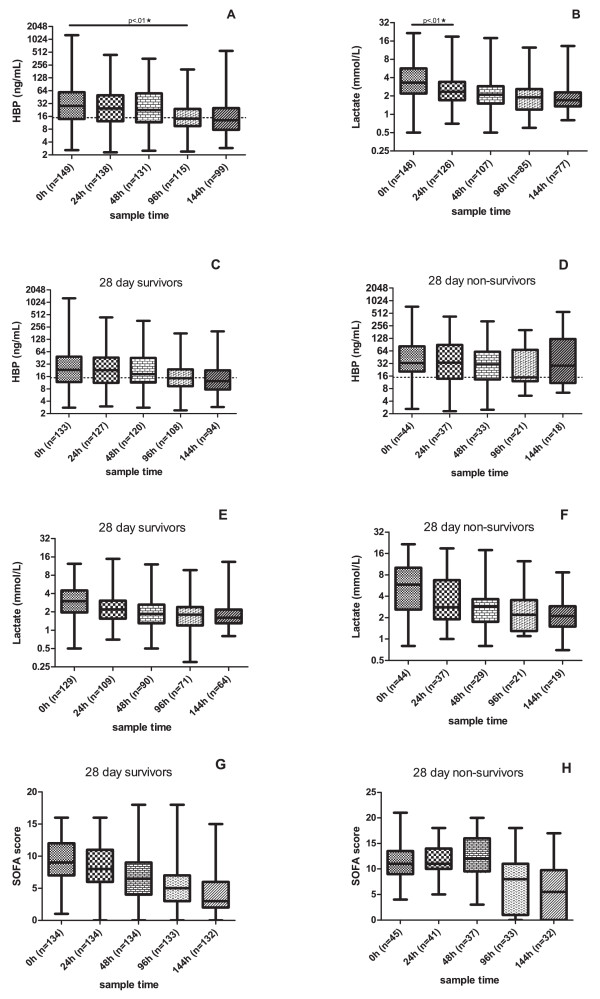
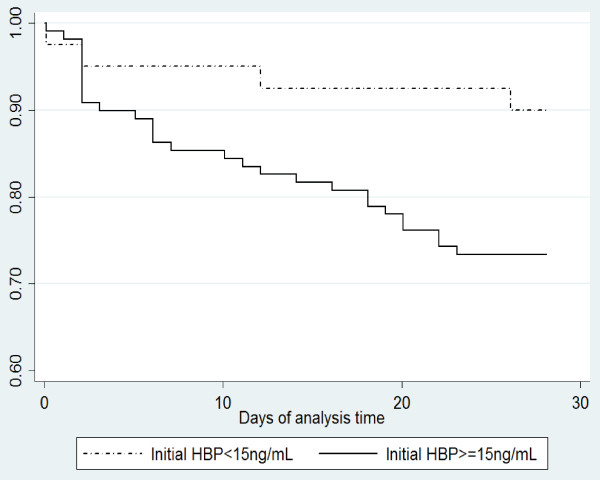
Results: HBP levels were significantly higher in the sepsis group as compared to the control group. At admission to the ICU, a plasma HBP concentration of ≥ 15 ng/mL and/or a HBP (ng/mL)/white blood cell count (109/L) ratio of >2 was found in 87.2% and 50.0% of critically ill patients with sepsis and non-septic illness, respectively. A lactate level of >2.5 mmol/L was detected in 64.9% and 56.0% of the same patient groups. Both in the sepsis group (n = 151) and in the whole group (n = 179), plasma HBP concentrations at admission and in the last measured sample within the 144 hour study period were significantly higher among 28-day non-survivors as compared to survivors and in the sepsis group, an elevated HBP-level at baseline was associated with an increased case-fatality rate at 28 days.
Conclusions: Plasma HBP levels were significantly higher in patients with severe sepsis or septic shock compared to patients with a non-septic illness in the ICU. HBP was associated with severity of disease and an elevated HBP at admission was associated with an increased risk of death. HBP that rises over time may identify patients with a deteriorating prognosis. Thus, repeated HBP measurement in the ICU may help monitor treatment and predict outcome in patients with severe infections.
Figures
Comment in
-
Should heparin-binding protein levels be routinely monitored in patients with severe sepsis and septic shock?Crit Care. 2012 Jun 28;16(3):133. doi: 10.1186/cc11379. Crit Care. 2012. PMID: 22748111 Free PMC article.
References
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 2008;34:17–60. doi: 10.1007/s00134-007-0934-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
