

doi: 10.1186/1741-7007-10-42.
Q&A: 'toxic' effects of sugar: should we be afraid of fructose?
Affiliations
- PMID: 22613805
- PMCID: PMC3357317
- DOI: 10.1186/1741-7007-10-42
Item in Clipboard
Q&A: 'toxic' effects of sugar: should we be afraid of fructose?
BMC Biol.
.
No abstract available
Figures

Digestion and absorption of starch and sugar. Starch is a polymer of several thousand molecules of glucose, which is digested by the pancreatic enzyme alpha-amylase into maltose, isomaltose, maltotriose (not represented in the figure) and maltodextrins. At the level of the brush border of the intestinal mucosa, specific enzymes generate glucose from maltose (sucrase, maltase), isomaltose (isomaltase) and maltodextrins (glucoamylase). Glucose is then absorbed into the enterocyte by an apical co-transport with NaCl (Sodium-glucose-transporter-1, SGLT1) and transferred to the blood at the basolateral membrane through a facilitated transport mediated by GLUT2. Sucrose is cleaved into glucose and fructose by sucrase at the brush border. Fructose is transported into the enterocyte independently of Na by GLUT5, and due to the presence of fructose metabolizing, gluconeogenic and lipogenic enzymes, part of the absorbed fructose may be metabolized to lactate, glucose, and fatty acids within the enterocytes. Unmetabolized fructose is transferred to the blood at the basolateral membrane by GLUT2.
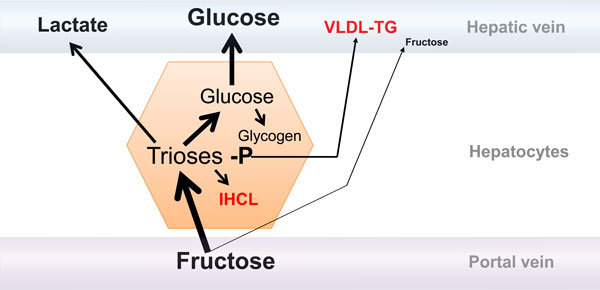
Metabolism of fructose in the liver. The majority of fructose in the portal vein is taken up by the liver to be converted into glucose, glycogen, and lactate. A small portion may be either oxidized within hepatocytes or converted into fatty acid, which will be either secreted as very low density lipoprotein-triglyceride (VLDL-TG) particles or stored as intrahepatocellular lipids (IHCL). Only a minor portion escapes liver uptake and reaches the systemic circulation; blood fructose concentrations therefore remain very low even after ingestion of a large fructose load.
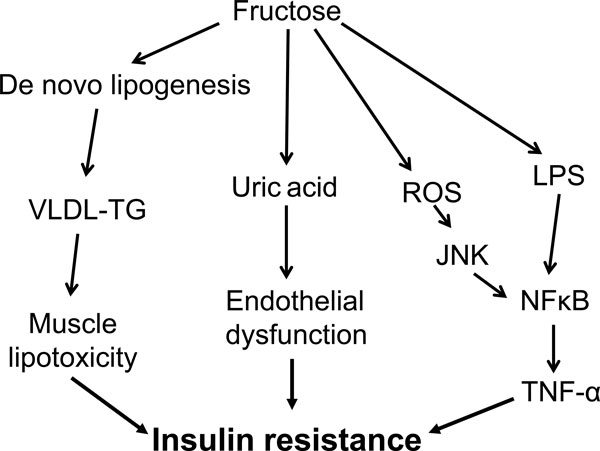
Putative mechanisms that may link excessive fructose intake to the development of metabolic disorders in the long term. Stimulation of hepatic de novo lipogenesis may lead to the deposition of fat within the liver, which may secondarily be involved in hepatic insulin resistance. Hepatic de novo lipogenesis may also cause an increase in VLDL-TG secretion and ectopic deposition of lipids in skeletal muscle, and contribute to muscle insulin resistance through the generation of muscle lipid metabolites. Fructose metabolism in the liver increases uric acid synthesis, and the ensuing hyperuricemia can secondarily be responsible for endothelial cell dysfunction, impaired insulin-induced vasodilation and a consequent failure to increase muscle blood flow after a meal, leading to muscle insulin resistance. In addition, the metabolism of fructose in liver cells can cause the formation of reactive oxygen species (ROS), which can activate nuclear factor (NF)κB, causing inflammation-linked insulin resistance. Finally, fructose can increase the translocation of bacterial endotoxin (lipopolysaccharide (LPS)) into the portal blood, causing endotoxin-mediated stimulation of inflammation. TNF, tumor necrosis factor.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
