

Model-based tomographic reconstruction of objects containing known components
- PMID: 22614574
- PMCID: PMC4503263
- DOI: 10.1109/TMI.2012.2199763
Model-based tomographic reconstruction of objects containing known components
Abstract
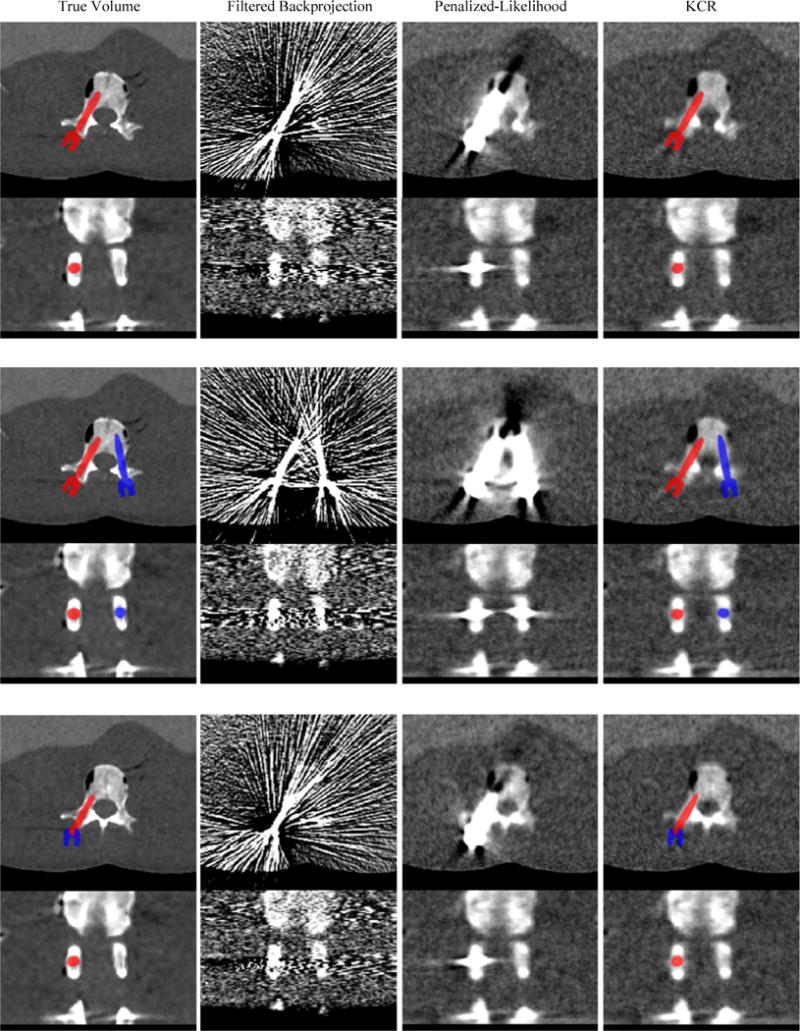
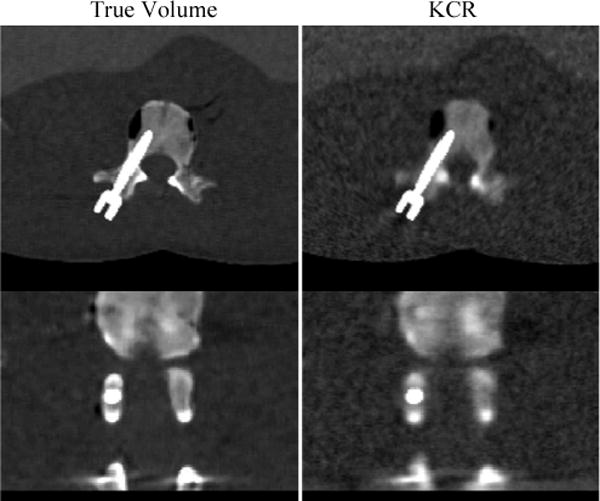
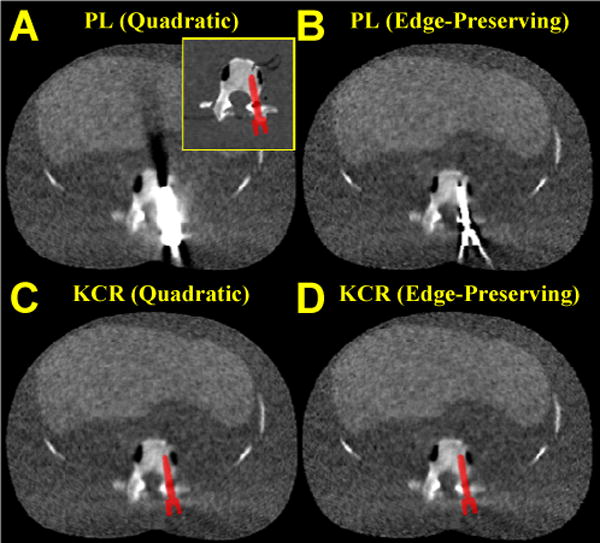
The likelihood of finding manufactured components (surgical tools, implants, etc.) within a tomographic field-of-view has been steadily increasing. One reason is the aging population and proliferation of prosthetic devices, such that more people undergoing diagnostic imaging have existing implants, particularly hip and knee implants. Another reason is that use of intraoperative imaging (e.g., cone-beam CT) for surgical guidance is increasing, wherein surgical tools and devices such as screws and plates are placed within or near to the target anatomy. When these components contain metal, the reconstructed volumes are likely to contain severe artifacts that adversely affect the image quality in tissues both near and far from the component. Because physical models of such components exist, there is a unique opportunity to integrate this knowledge into the reconstruction algorithm to reduce these artifacts. We present a model-based penalized-likelihood estimation approach that explicitly incorporates known information about component geometry and composition. The approach uses an alternating maximization method that jointly estimates the anatomy and the position and pose of each of the known components. We demonstrate that the proposed method can produce nearly artifact-free images even near the boundary of a metal implant in simulated vertebral pedicle screw reconstructions and even under conditions of substantial photon starvation. The simultaneous estimation of device pose also provides quantitative information on device placement that could be valuable to quality assurance and verification of treatment delivery.
Figures

References
-
- De Man B, et al. Metal streak artifacts in X-ray computed tomography: A simulation study. IEEE Trans Nuclear Science. 1999;46:691–696.
-
- Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. Radiographics. 2004 Nov-Dec;24:1679–91. - PubMed
-
- Stulberg SD, et al. Monitoring pelvic osteolysis following total hip replacement surgery: an algorithm for surveillance. J Bone Joint Surg Am. 2002;84-A(Suppl 2):116–22. - PubMed
-
- Holly LT, Foley KT. Three-dimensional fluoroscopy-guided percutaneous thoracolumbar pedicle screw placement. Technical note. J Neurosurg. 2003 Oct;99:324–9. - PubMed
-
- Wang MY, et al. Reliability of three-dimensional fluoroscopy for detecting pedicle screw violations in the thoracic and lumbar spine. Neurosurgery. 2004 May;54:1138–42. discussion 1142–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
