

What is personalized medicine and what should it replace?
- PMID: 22614753
- PMCID: PMC3684057
- DOI: 10.1038/nrgastro.2012.100
What is personalized medicine and what should it replace?
Abstract
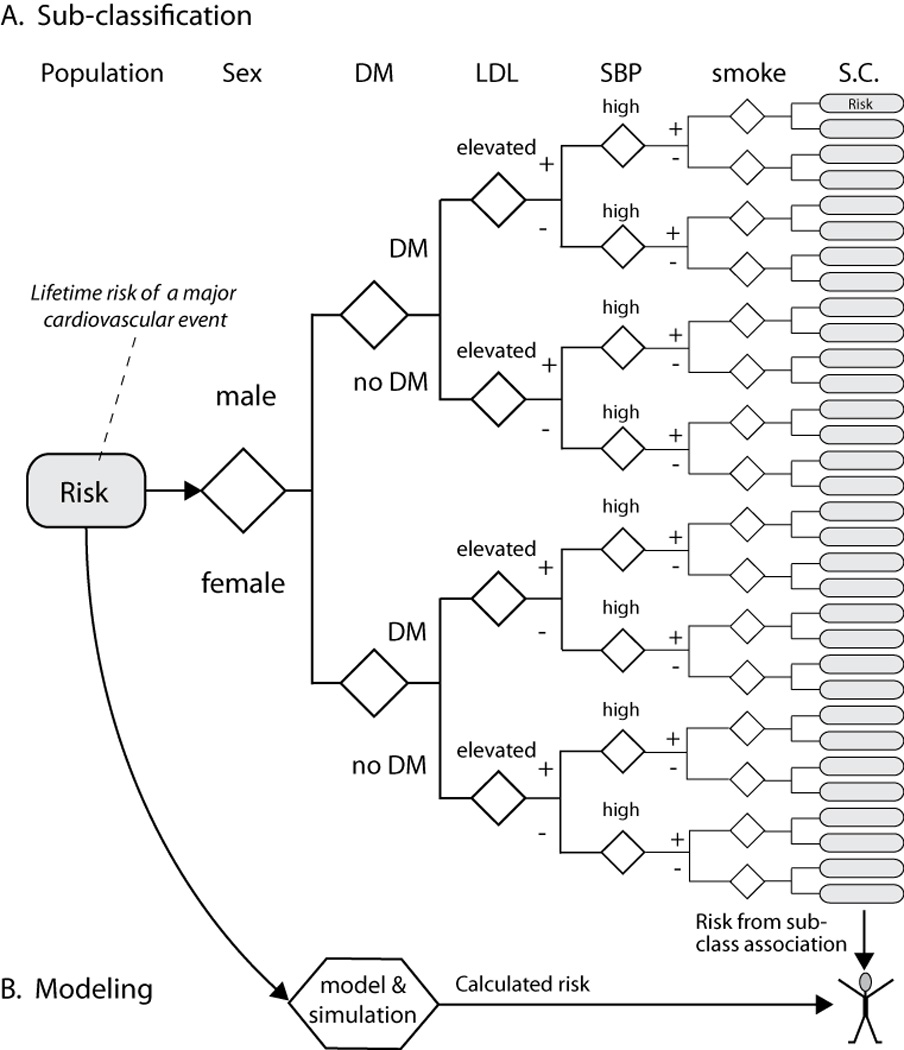
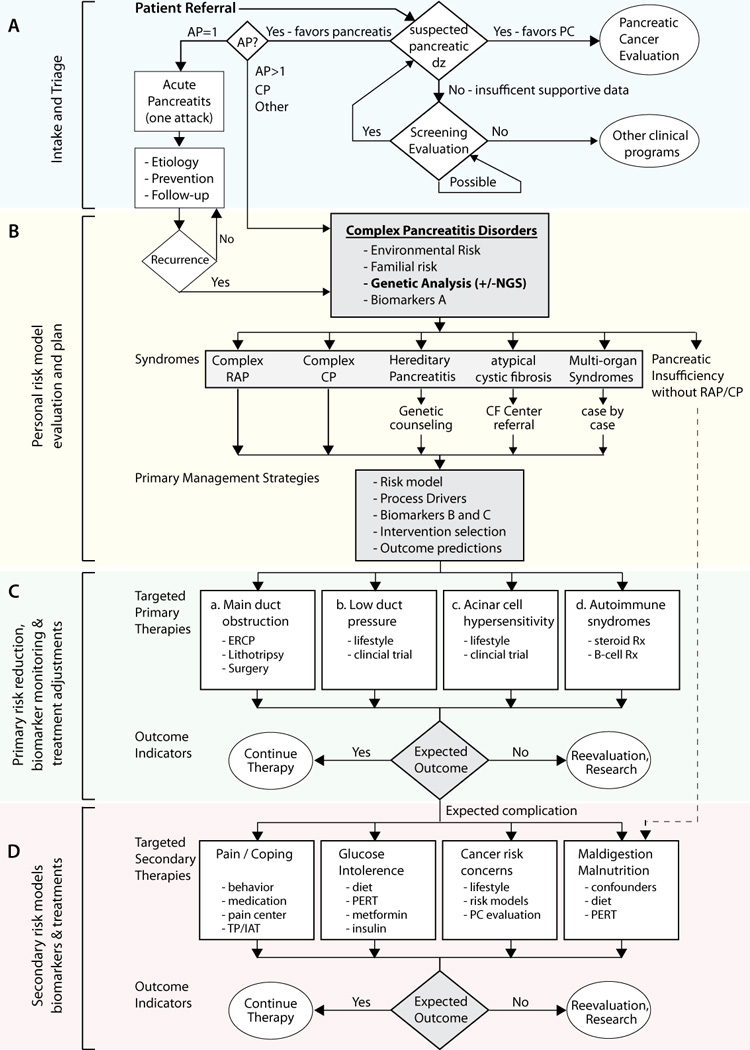
Personalized medicine is a new framework for medical care that involves modelling and simulation of a disease on the basis of its underlying mechanisms. This strategy must replace the 20(th) century paradigm of defining disease by pathology or associated signs and symptoms and conducting outcomes research that is based on the presence or absence of the disease syndrome. New technologies, including next-generation sequencing, the 'omics' and powerful computers provide massive amounts of accurate data. However, attempts to understand complex disorders by applying these new technologies within the 20(th) century framework have failed to produce the expected medical advances. To help physicians embrace a paradigm shift, the limitations of the old framework and major advantages of the new framework must be demonstrated. Chronic pancreatitis is an ideal complex disorder to study to consider the pros and cons of the two frameworks, because the pancreas is such a simple organ for disease modelling, and the advantages of personalized medicine are so profound.
Figures
Comment in
-
Biopsy and personalized medicine.Nat Rev Gastroenterol Hepatol. 2012 Nov;9(11):683; author reply 683. doi: 10.1038/nrgastro.2012.100-c1. Epub 2012 Oct 2. Nat Rev Gastroenterol Hepatol. 2012. PMID: 23026901 Free PMC article. No abstract available.
References
-
- Kuhn TS. The Structure of Scientific Revolutions. 1st. ed ed. Chicago: Univ. of Chicago; 1962.
-
- Committee on a Framework for Development a New Taxonomy of Disease; National Research Council. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease. Washington, DC: National Academies Press; - PubMed
-
- Flexner A. Medical Education in the United States and Candida: A report to the Carnegie Foundation for the Advancement of teaching. Boston: Mass; 1910.
-
- Etemad B, Whitcomb DC. Chronic pancreatitis: Diagnosis, classification, and new genetic developments. Gastroenterology. 2001;120:682–707. - PubMed
-
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. New England Journal of Medicine. 1995;332(22):1482–1490. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
