

Diagnosis and management of hyponatremia in cancer patients
- PMID: 22618570
- PMCID: PMC3380874
- DOI: 10.1634/theoncologist.2011-0400
Diagnosis and management of hyponatremia in cancer patients
Abstract
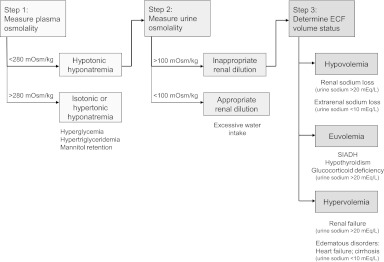
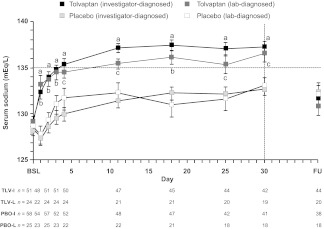
Hyponatremia, a common electrolyte abnormality in oncology practice, may be a negative prognostic factor in cancer patients based on a systematic analysis of published studies. The largest body of evidence comes from small-cell lung cancer (SCLC), for which hyponatremia was identified as an independent risk factor for poor outcome in six of 13 studies. Hyponatremia in the cancer patient is usually caused by the syndrome of inappropriate antidiuretic hormone (SIADH), which develops more frequently with SCLC than with other malignancies. SIADH may be driven by ectopic production of arginine vasopressin (AVP) by tumors or by effects of anticancer and palliative medications on AVP production or action. Other factors may cause hypovolemic hyponatremia, including diarrhea and vomiting caused by cancer therapy. Hyponatremia may be detected on routine laboratory testing before or during cancer treatment or may be suggested by the presence of mostly neurological symptoms. Treatment depends on several factors, including symptom severity, onset timing, and extracellular volume status. Appropriate diagnosis is important because treatment differs by etiology, and choosing the wrong approach can worsen the electrolyte abnormality. When hyponatremia is caused by SIADH, hypertonic saline is indicated for acute, symptomatic cases, whereas fluid restriction is recommended to achieve a slower rate of correction for chronic asymptomatic hyponatremia. Pharmacological therapy may be necessary when fluid restriction is insufficient. The orally active, selective AVP receptor 2 (V(2))-receptor antagonist tolvaptan provides a mechanism-based option for correcting hyponatremia caused by SIADH or other conditions with inappropriate AVP elevations. By blocking AVP effects in the renal collecting duct, tolvaptan promotes aquaresis, leading to a controlled increase in serum sodium levels.
Conflict of interest statement
Figures
References
-
- Palmer BF, Gates JR, Lader M. Causes and management of hyponatremia. Ann Pharmacother. 2003;37:1694–1702. - PubMed
-
- Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000;342:1581–1589. - PubMed
-
- Lassen U, Østerlind K, Hansen M, et al. Long-term survival in small-cell lung cancer: Posttreatment characteristics in patients surviving 5 to 18+ years—an analysis of 1,714 consecutive patients. J Clin Oncol. 1995;13:1215–1220. - PubMed
-
- Østerlind K, Andersen PK. Prognostic factors in small cell lung cancer: Multivariate model based on 778 patients treated with chemotherapy with or without irradiation. Cancer Res. 1986;46:4189–4194. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
