

Complications of Uterine Fibroids and Their Management, Surgical Management of Fibroids, Laparoscopy and Hysteroscopy versus Hysterectomy, Haemorrhage, Adhesions, and Complications
- PMID: 22619681
- PMCID: PMC3348525
- DOI: 10.1155/2012/791248
Complications of Uterine Fibroids and Their Management, Surgical Management of Fibroids, Laparoscopy and Hysteroscopy versus Hysterectomy, Haemorrhage, Adhesions, and Complications
Abstract
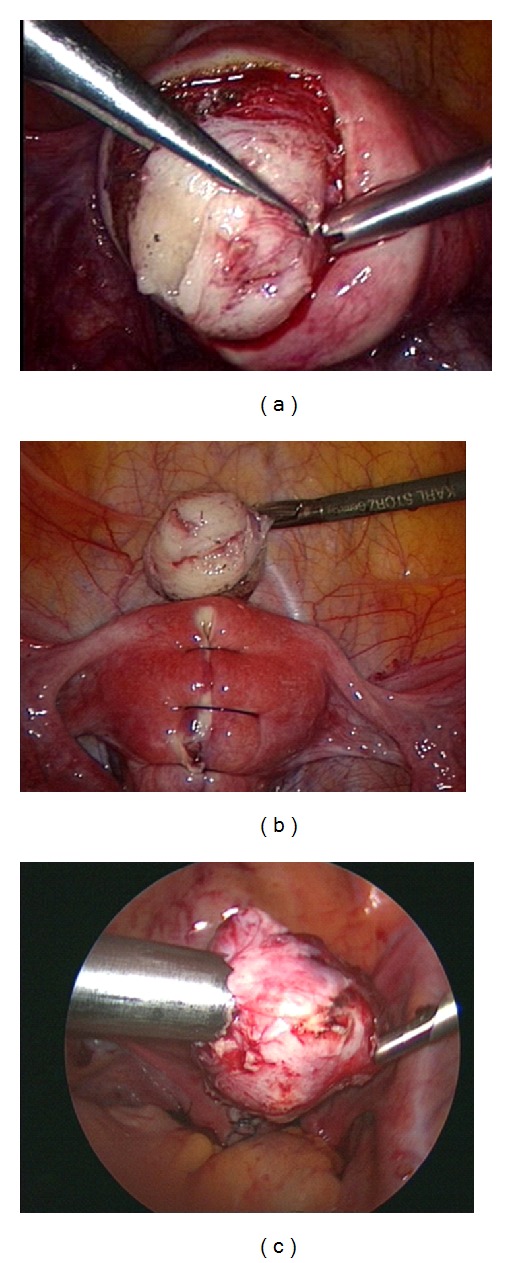
A critical analysis of the surgical treatment of fibroids compares all available techniques of myomectomy. Different statistical analyses reveal the advantages of the laparoscopic and hysteroscopic approach. Complications can arise from the location of the fibroids. They range from intermittent bleedings to continuous bleedings over several weeks, from single pain episodes to severe pain, from dysuria and constipation to chronic bladder and bowel spasms. Very seldom does peritonitis occur. Infertility may result from continuous metro and menorrhagia. The difficulty of the laparoscopic and hysteroscopic myomectomy lies in achieving satisfactory haemostasis using the appropriate sutures. The hysteroscopic myomectomy requires an operative hysteroscope and a well-experienced gynaecologic surgeon.
Figures
References
-
- Semm K, Mettler L. Technical progress in pelvic surgery via operative laparoscopy. American Journal of Obstetrics and Gynecology. 1980;138(2):121–127. - PubMed
-
- Figdor PP. Philipp Bozzini: der Beginn der modernen Endoskopie : die Wiener und Frankfurter “Bozzini-Akte” und Publikationen der Jahre 1805 bis 1807. Endo-Press; 2002.
-
- Lindemann HJ. CO2-hysteroscopy today. Endoscopy. 1979;11(2):94–100. - PubMed
-
- Bettocchi S, Di Spiezio Sardo A, Ceci O, et al. A new hysteroscopic technique for the preparation of partially intramural myomas in office setting (OPPIuM technique): a pilot study. Journal of Minimally Invasive Gynecology. 2009;16(6):748–754. - PubMed
-
- Loffer FD, Bradley LD, Brill AI, et al. Hysteroscopic fluid monitoring guidelines. The ad hoc committee on hysteroscopic training guidelines of the American Association of Gynecologic Laparoscopists. The Journal of the American Association of Gynecologic Laparoscopists. 2007;7(1):167–168. - PubMed
LinkOut - more resources
Full Text Sources
Medical
