

Local-regional control according to surrogate markers of breast cancer subtypes and response to neoadjuvant chemotherapy in breast cancer patients undergoing breast conserving therapy
- PMID: 22621334
- PMCID: PMC3446346
- DOI: 10.1186/bcr3198
Local-regional control according to surrogate markers of breast cancer subtypes and response to neoadjuvant chemotherapy in breast cancer patients undergoing breast conserving therapy
Abstract
Introduction: Breast cancers of different molecular subtypes have different survival rates. The goal of this study was to identify patients at high risk for local-regional recurrence according to response to neoadjuvant chemotherapy and surrogate markers of molecular subtypes in patients undergoing breast conserving therapy (BCT).
Methods: Clinicopathologic data from 595 breast cancer patients who received neoadjuvant chemotherapy and BCT from 1997 to 2005 were identified. Estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) expression determined by immunohistochemistry were used to construct the following subtypes: ER+ or PR+ and HER2- (hormone receptor (HR)+/HER2-; 52%), ER+ or PR+ and HER2+ (HR+/HER2+; 9%), ER- and PR- and HER2+ (HR-/HER2+; 7%) and ER- and PR- and HER2- (HR-/HER2-; 32%). Actuarial rates were calculated using the Kaplan-Meier method and compared using the log-rank test. Cox proportional hazards models were used for multivariate analysis (MVA).
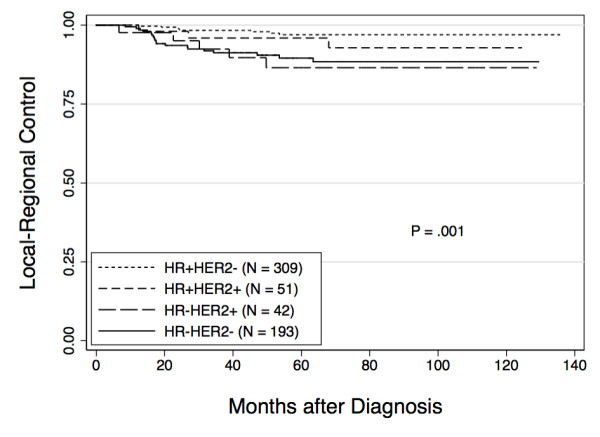
Results: After a median follow-up of 64 months, the five-year local-regional recurrence (LRR)-free survival rate for all patients was 93.8%. The five-year LRR-free survival rates varied by subtype: HR+/HER2- 97.0%, HR+/HER2+ 95.9%, HR-/HER2+ 86.5% and HR-/HER2- 89.5% (P = 0.001). In addition to subtype, clinical stage III disease (90% vs. 95% for I/II, P = 0.05), high nuclear grade (92% vs. 97% with low/intermediate grade, P = 0.03), presence of lymphovascular invasion (LVI) (89% vs. 95% in those without LVI, P = 0.02) and four or more positive lymph nodes on pathologic examination (87% vs. 95% with zero to three positive lymph nodes, P = 0.03) were associated with lower five-year LRR-free survival on univariate analysis. On MVA, HR-/HER2+ and HR-/HER2- subtypes and disease in four or more lymph nodes were associated with decreased LRR-free survival. A pathologic complete response (pCR) was associated with improved LRR-free survival.
Conclusions: Patients with HR+/HER2- and HR+/HER2+ subtypes had excellent LRR-free survival regardless of tumor response to neoadjuvant chemotherapy. Patients with HR-/HER2+ and HR-/HER2- subtypes with poor response to neoadjuvant chemotherapy had worse LRR-free survival after BCT. Additional study is needed to determine the impact of trastuzumab on local-regional control in HER2+ tumors. Our data suggest that patients with HR-/HER2- subtype tumors not achieving pCR may benefit from novel strategies to improve local-regional control.
Figures
References
-
- Arriagada R, Le MG, Rochard F, Contesso G. Conservative treatment versus mastectomy in early breast cancer: patterns of failure with 15 years of follow-up data. Institut Gustave-Roussy Breast Cancer Group. J Clin Oncol. 1996;14:1558–1564. - PubMed
-
- Blichert-Toft M, Rose C, Andersen JA, Overgaard M, Axelsson CK, Andersen KW, Mouridsen HT. Danish randomized trial comparing breast conservation therapy with mastectomy: six years of life-table analysis. Danish Breast Cancer Cooperative Group. J Natl Cancer Inst Monogr. 1992. pp. 19–25. - PubMed
-
- Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, Jeong JH, Wolmark N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–1241. doi: 10.1056/NEJMoa022152. - DOI - PubMed
-
- Poggi MM, Danforth DN, Sciuto LC, Smith SL, Steinberg SM, Liewehr DJ, Menard C, Lippman ME, Lichter AS, Altemus RM. Eighteen-year results in the treatment of early breast carcinoma with mastectomy versus breast conservation therapy: the National Cancer Institute Randomized Trial. Cancer. 2003;98:697–702. doi: 10.1002/cncr.11580. - DOI - PubMed
-
- van Dongen JA, Voogd AC, Fentiman IS, Legrand C, Sylvester RJ, Tong D, van der Schueren E, Helle PA, van Zijl K, Bartelink H. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 2000;92:1143–1150. doi: 10.1093/jnci/92.14.1143. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
