

Associations of plasma 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D concentrations with death and progression to maintenance dialysis in patients with advanced kidney disease
- PMID: 22621970
- PMCID: PMC3439559
- DOI: 10.1053/j.ajkd.2012.04.014
Associations of plasma 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D concentrations with death and progression to maintenance dialysis in patients with advanced kidney disease
Abstract
Background: Low vitamin D concentrations are prevalent in patients with chronic kidney disease (CKD). We investigated the relationship between plasma 25-hydroxyvitamin D (25[OH]D) or 1,25-dihydroxyvitamin D (1,25[OH](2)D) concentrations with death, cardiovascular events, and dialysis therapy initiation in patients with advanced CKD.
Study design: The HOST (Homocysteinemia in Kidney and End Stage Renal Disease) Study was a randomized double-blind trial evaluating the effects of high doses of folic acid on death and long-term dialysis therapy initiation in patients with advanced CKD (stages 4 and 5 not yet on dialysis therapy). 25(OH)D and 1,25(OH)(2)D were measured in stored plasma samples obtained 3 months after trial initiation and evaluated at clinically defined cutoffs (<10, 10-30, and >30 ng/mL) and tertiles (<15, 15-22, and >22 pg/mL), respectively. Cox proportional hazard models were used to examine the association between vitamin D concentrations and clinical outcomes.
Setting & participants: 1,099 patients with advanced CKD from 36 Veteran Affairs Medical Centers.
Predictors: 25(OH)D and 1,25(OH)(2)D concentrations.
Outcomes: Death, cardiovascular events, and time to initiation of long-term dialysis therapy.
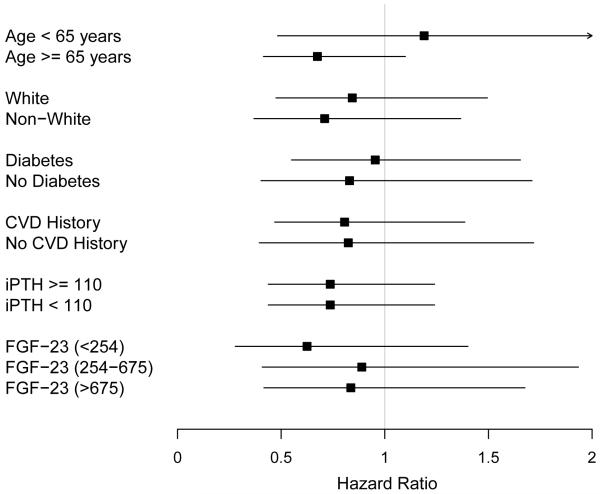
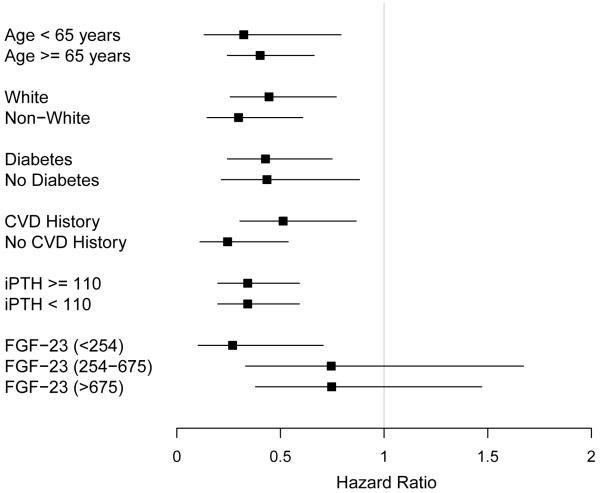
Results: After a median follow-up of 2.9 years, 41% (n = 453) died, whereas 56% (n = 615) initiated dialysis therapy. Mean 25(OH)D and 1,25(OH)(2)D concentrations were 21 ± 10 ng/mL and 20 ± 11 pg/mL, respectively. After adjustment for potential confounders, the lowest tertile of 1,25(OH)(2)D was associated with death (HR, 1.33; 95% CI, 1.01-1.74) and initiation of long-term dialysis therapy (HR, 1.78; 95% CI, 1.40-2.26) compared with the highest tertile. The association with death and initiation of dialysis therapy was moderately attenuated after adjustment for plasma fibroblast growth factor 23 (FGF-23) concentrations (HRs of lower tertiles of 1.20 [95% CI, 0.91-1.58] and 1.56 [95% CI, 1.23-1.99], respectively, compared with highest tertile). There was no association between 25(OH)D concentrations and outcomes.
Limitations: Participants were mostly men.
Conclusions: Low plasma 1,25(OH)(2)D concentrations are associated with death and initiation of long-term dialysis therapy in patients with advanced CKD. FGF-23 level may attentuate this relationship.
Copyright © 2012 National Kidney Foundation, Inc. All rights reserved.
Figures
References
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–2047. - PubMed
-
- Keith DS, Nichols GA, Guillon CM, Brown JB, Smith DH. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Internal Med. 2004;164(6):659–663. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. - PubMed
-
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–81. - PubMed
-
- Holick MF. Vitamin D for health and in chronic kidney disease. Semin Dial. 2005;18(4):266–275. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
