

The serum anion gap is altered in early kidney disease and associates with mortality
- PMID: 22622500
- PMCID: PMC3434284
- DOI: 10.1038/ki.2012.196
The serum anion gap is altered in early kidney disease and associates with mortality
Abstract
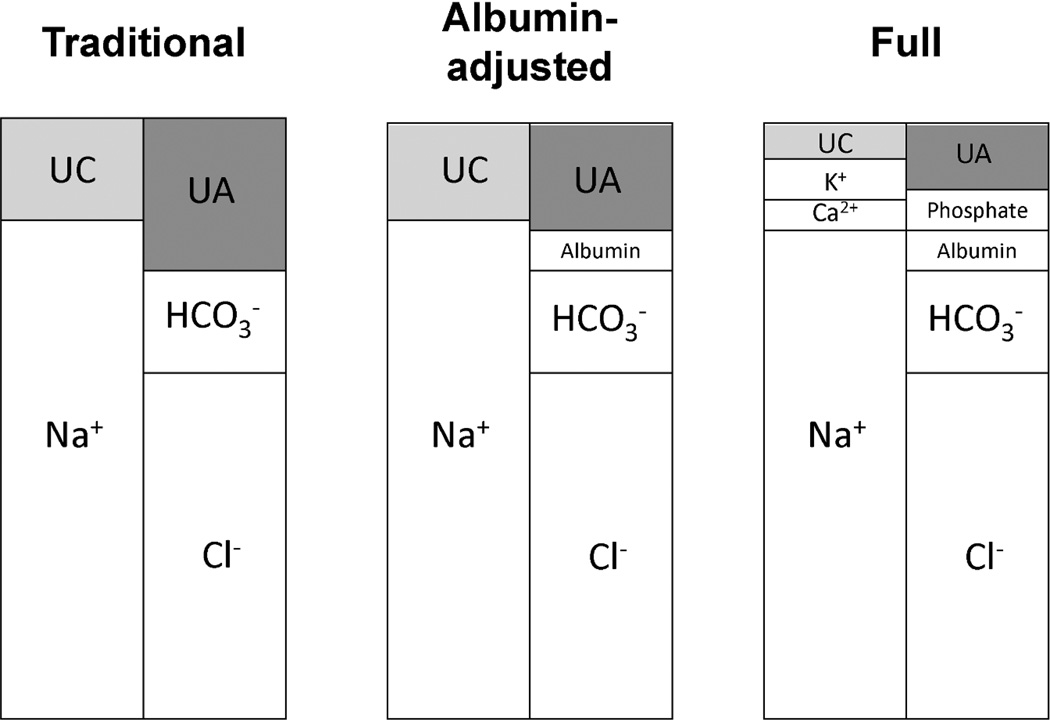
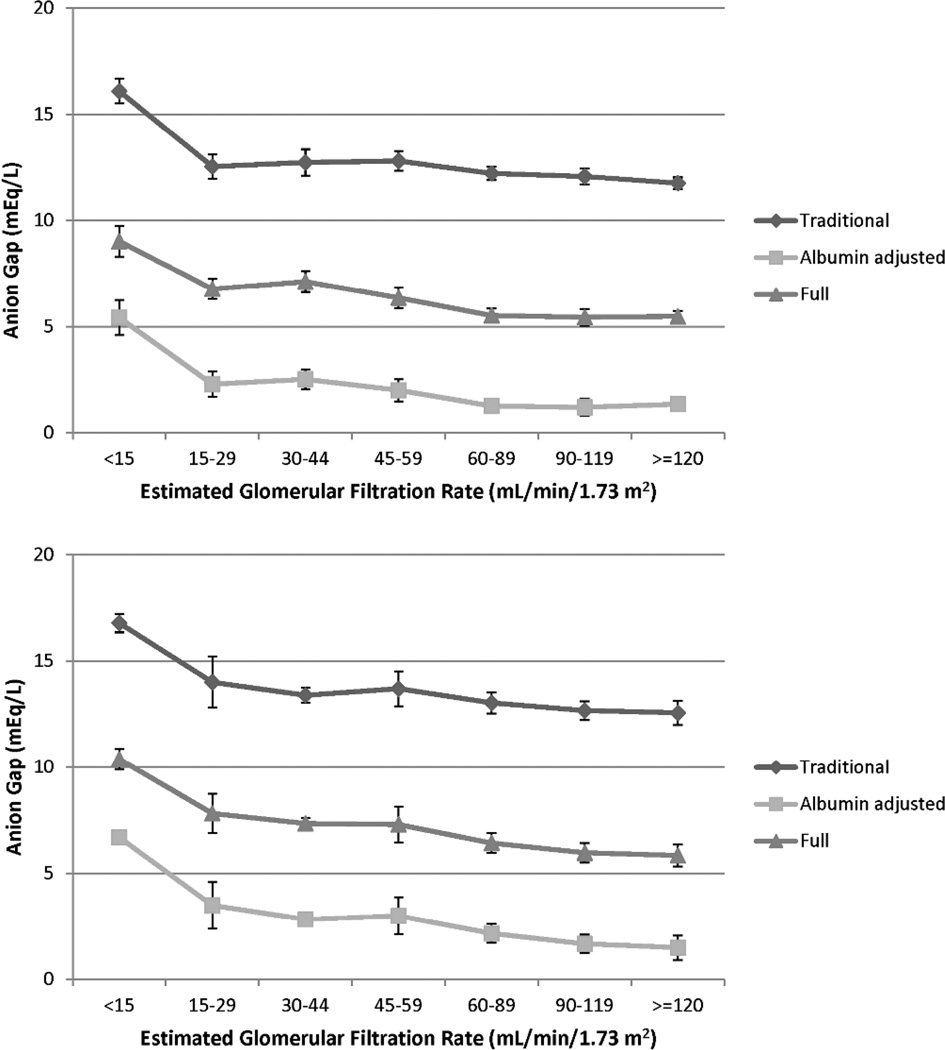
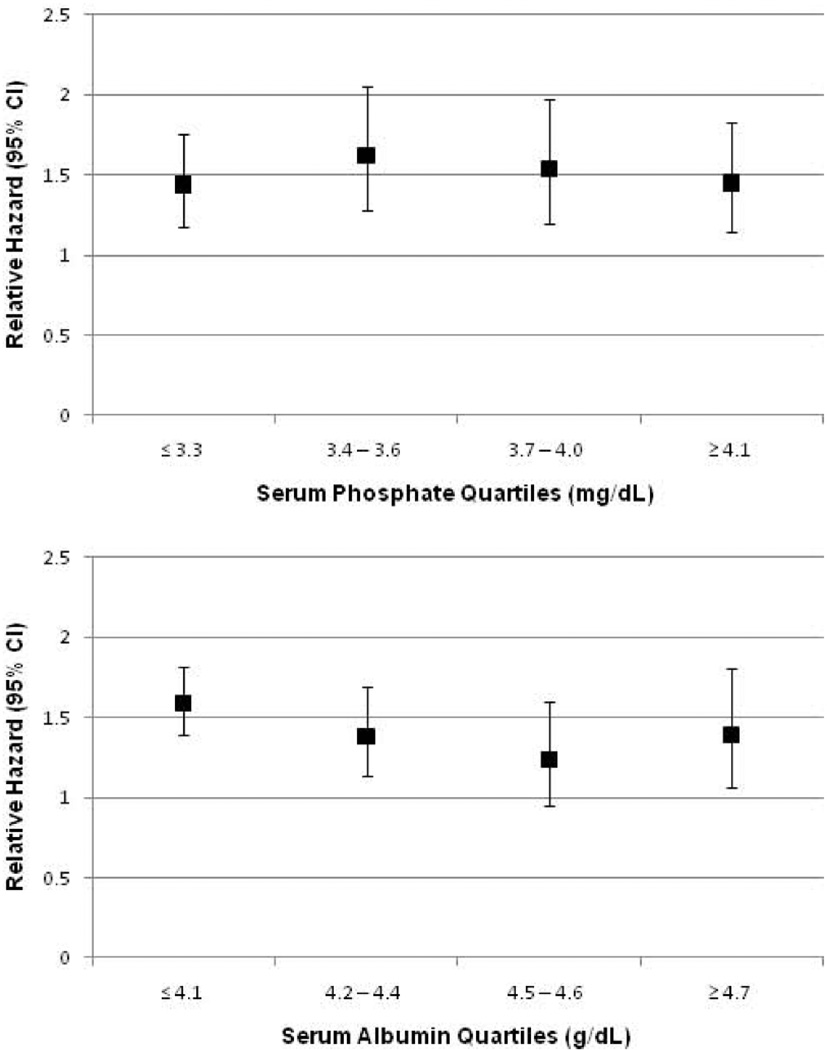
It is well known that uremia causes an increase in the serum anion gap (AG); however, whether changes in the AG occur earlier in the course of chronic kidney disease is not known. Here we investigated whether different measures of the AG, as a marker of kidney function, are associated with mortality. To do this, we analyzed the available laboratory data of 11,957 adults in the National Health and Nutrition Examination Survey 1999-2004 to calculate AG using the traditional method, or one that was albumin-adjusted, as well as a full AG reflecting other electrolytes. A significant elevation in the traditional AG was seen only with an estimated glomerular filtration rate (eGFR) <45 ml/min per 1.73 m(2), whereas increases in the albumin-adjusted and full AG were found with eGFRs <60 or 90 ml/min per 1.73 m(2), respectively. Higher levels of each AG were associated with an increased risk of all-cause mortality after adjustment for age, gender, race/ethnicity, and eGFR. After adjustment for additional covariates including body mass index and comorbidities, higher levels of the albumin-adjusted and full AG were associated with mortality (relative hazard for the highest compared with the lowest quartile were 1.62 and 1.64, respectively). Thus, higher levels of AG are present in individuals with less advanced kidney disease than previously recognized, and are associated with increased risk of mortality. Further study is needed to identify the unmeasured anions and to determine their physiological significance.
Conflict of interest statement
Dr. Hostetter has consulted for Bristol Myers Squibb, Eli Lilly, Genzyme, and Wyeth. Neither of the other authors has any financial conflicts to disclose.
Figures
Comment in
-
Risk factors: filling in the gap.Nat Rev Nephrol. 2012 Oct;8(10):562-3. doi: 10.1038/nrneph.2012.188. Epub 2012 Aug 14. Nat Rev Nephrol. 2012. PMID: 22890182 No abstract available.
-
Unmeasured anions and cations in advanced chronic kidney disease.Kidney Int. 2013 Aug;84(2):413-4. doi: 10.1038/ki.2013.182. Kidney Int. 2013. PMID: 23903424 No abstract available.
-
The authors reply.Kidney Int. 2013 Aug;84(2):414-5. doi: 10.1038/ki.2013.183. Kidney Int. 2013. PMID: 23903425 No abstract available.
References
-
- Hakim RM, Lazarus JM. Biochemical parameters in chronic renal failure. Am J Kidney Dis. 1988;11:238–247. - PubMed
-
- Wallia R, Greenberg A, Piraino B, et al. Serum electrolyte patterns in end-stage renal disease. Am J Kidney Dis. 1986;8:98–104. - PubMed
-
- Widmer B, Gerhardt RE, Harrington JT, et al. Serum electrolyte and acid base composition. The influence of graded degrees of chronic renal failure. Arch Intern Med. 1979;139:1099–1102. - PubMed
-
- Eustace JA, Astor B, Muntner PM, et al. Prevalence of acidosis and inflammation and their association with low serum albumin in chronic kidney disease. Kidney Int. 2004;65:1031–1040. - PubMed
-
- Hsu CY, Chertow GM. Elevations of serum phosphorus and potassium in mild to moderate chronic renal insufficiency. Nephrol Dial Transplant. 2002;17:1419–1425. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R21DK077326/DK/NIDDK NIH HHS/United States
- R01 DK080123/DK/NIDDK NIH HHS/United States
- R01 DK087783/DK/NIDDK NIH HHS/United States
- TL1 RR025748/RR/NCRR NIH HHS/United States
- K23 DK078774/DK/NIDDK NIH HHS/United States
- KL2 RR025749/RR/NCRR NIH HHS/United States
- K23DK078774/DK/NIDDK NIH HHS/United States
- UL1 RR025750/RR/NCRR NIH HHS/United States
- R01DK080123/DK/NIDDK NIH HHS/United States
- UL1RR025750/RR/NCRR NIH HHS/United States
- R21 DK077326/DK/NIDDK NIH HHS/United States
- TL1RR025748/RR/NCRR NIH HHS/United States
- R01DK087783/DK/NIDDK NIH HHS/United States
- KL2RR025749/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
