

Modeling the dynamic relationship between HIV and the risk of drug-resistant tuberculosis
- PMID: 22623743
- PMCID: PMC3387814
- DOI: 10.1126/scitranslmed.3003815
Modeling the dynamic relationship between HIV and the risk of drug-resistant tuberculosis
Abstract
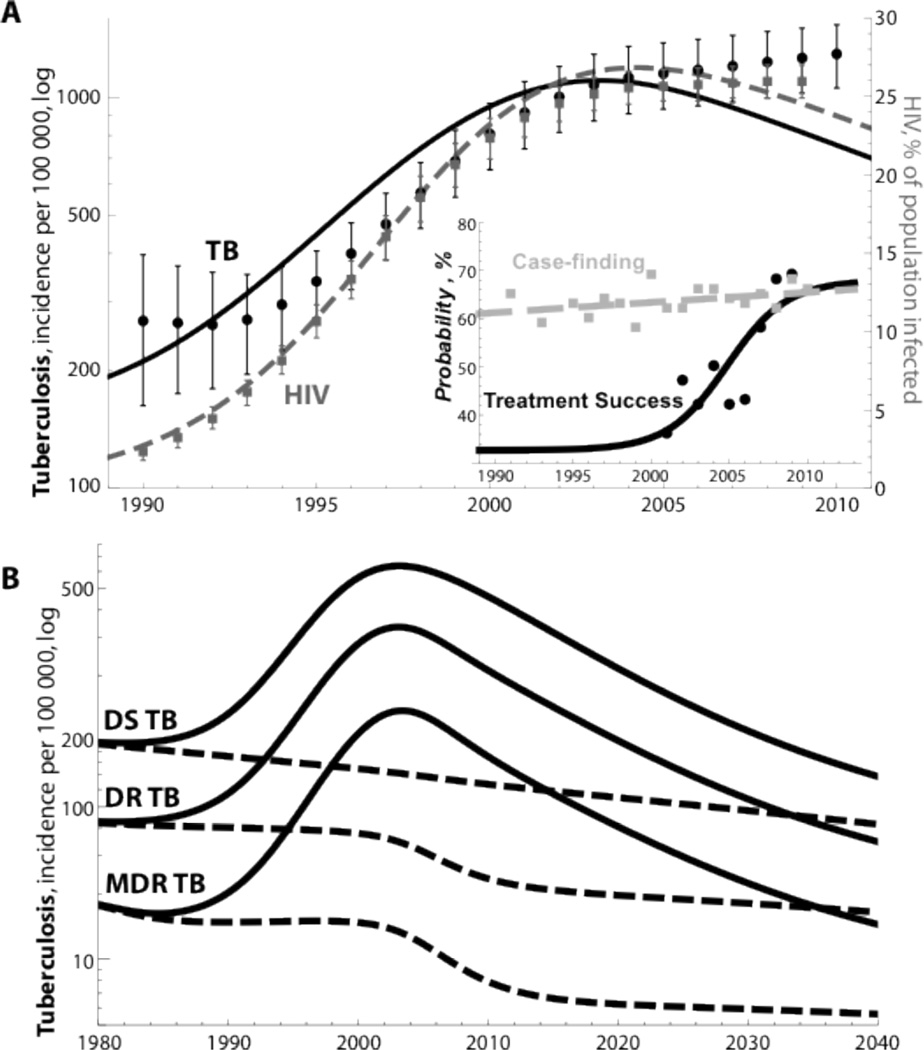
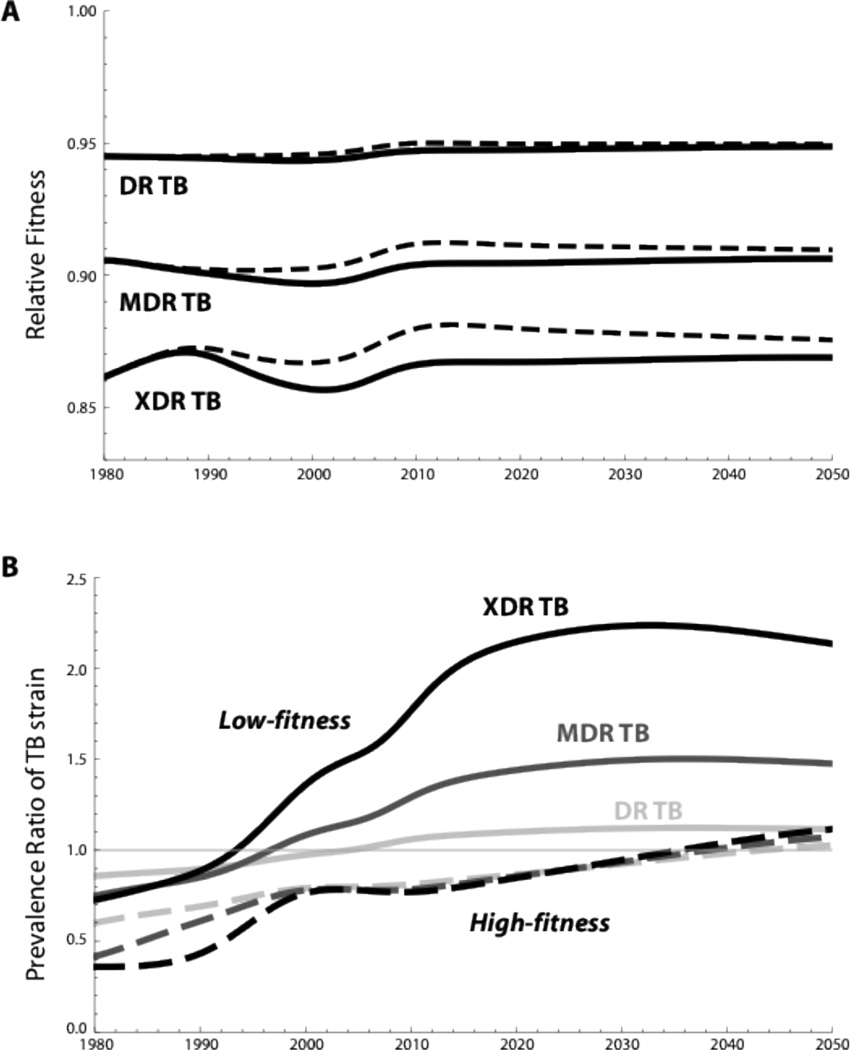
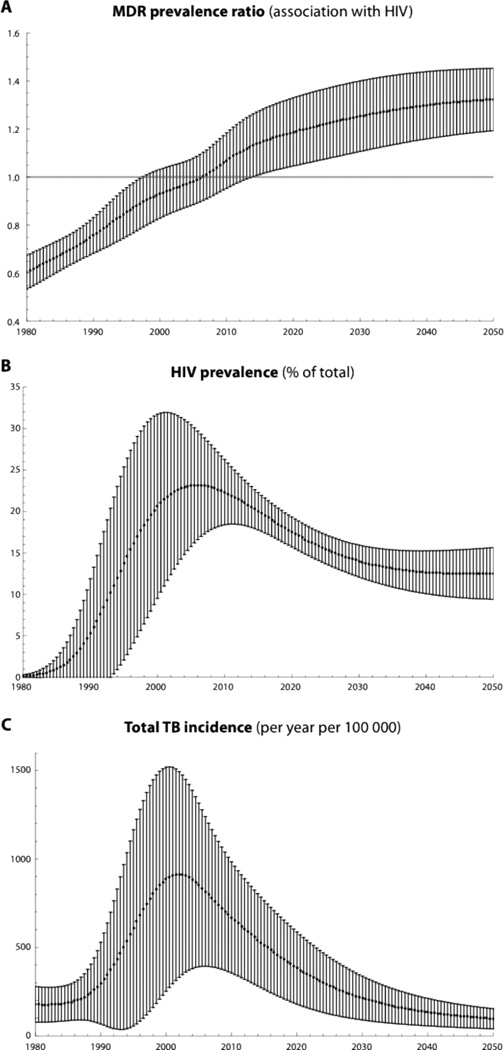
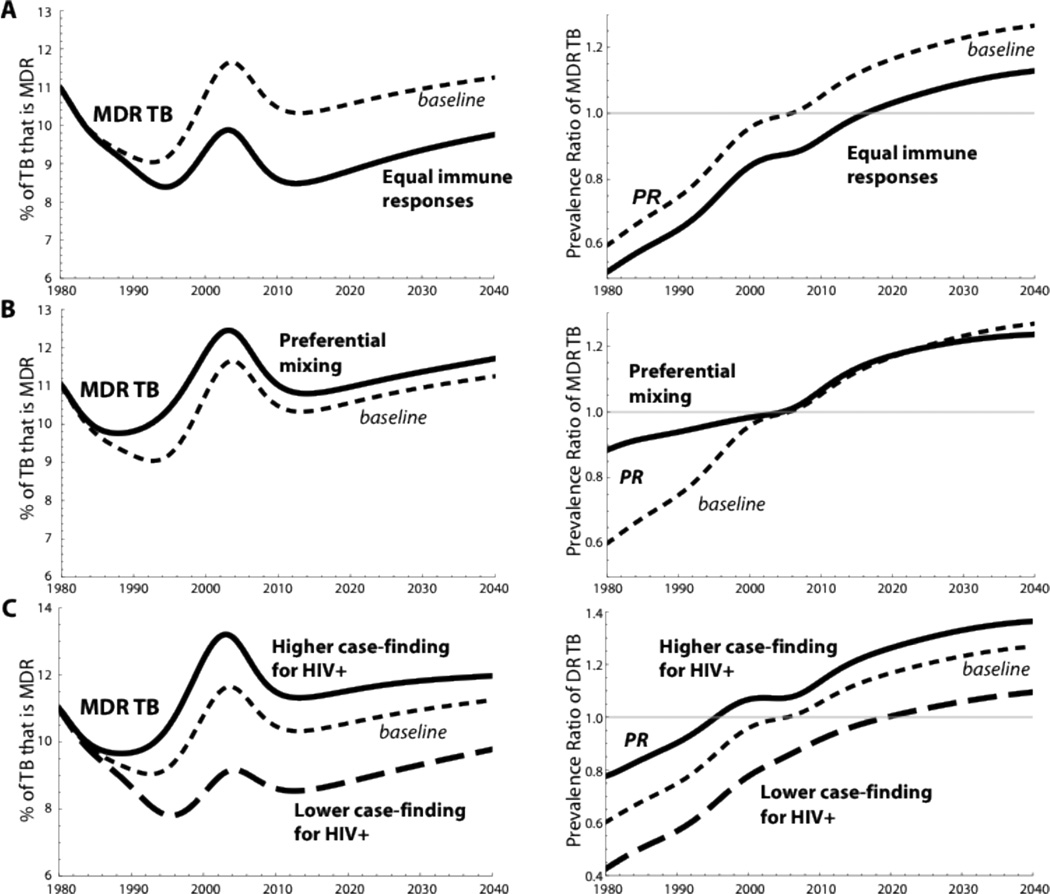
The emergence of highly drug-resistant tuberculosis (TB) and interactions between TB and HIV epidemics pose serious challenges for TB control. Previous researchers have presented several hypotheses for why HIV-coinfected TB patients may suffer an increased risk of drug-resistant TB (DRTB) compared to other TB patients. Although some studies have found a positive association between an individual's HIV status and his or her subsequent risk of multidrug-resistant TB (MDRTB), the observed individual-level relationship between HIV and DRTB varies substantially among settings. Here, we develop a modeling framework to explore the effect of HIV on the dynamics of DRTB. The model captures the acquisition of resistance to important classes of TB drugs, imposes fitness costs associated with resistance-conferring mutations, and allows for subsequent restoration of fitness because of compensatory mutations. Despite uncertainty in several key parameters, we demonstrate epidemic behavior that is robust over a range of assumptions. Whereas HIV facilitates the emergence of MDRTB within a community over several decades, HIV-seropositive individuals presenting with TB may, counterintuitively, be at lower risk of drug-resistant TB at early stages of the co-epidemic. This situation arises because many individuals with incident HIV infection will already harbor latent Mycobacterium tuberculosis infection acquired at an earlier time when drug resistance was less prevalent. We find that the rise of HIV can increase the prevalence of MDRTB within populations even as it lowers the average fitness of circulating MDRTB strains compared to similar populations unaffected by HIV. Preferential social mixing among individuals with similar HIV status and lower average CD4 counts among HIV-seropositive individuals further increase the expected burden of MDRTB. This model suggests that the individual-level association between HIV and drug-resistant forms of TB is dynamic, and therefore, cross-sectional studies that do not report a positive individual-level association will not provide assurance that HIV does not exacerbate the burden of resistant TB in the community.
Figures



Comment in
-
TB and HIV: deadly liaison or manageable threat?Sci Transl Med. 2012 May 23;4(135):135fs15. doi: 10.1126/scitranslmed.3004079. Sci Transl Med. 2012. PMID: 22623735
References
-
- Global tuberculosis control 2011. Geneva, Switzerland: WHO report, World Health Organization; 2011.
-
- Getahun H, Gunneberg C, Granich R, Nunn P. HIV Infection-Associated Tuberculosis: The Epidemiology and the Response. Clinical Infectious Diseases. 2010;50:S201–S207. - PubMed
-
- Wells CD, Cegielski JP, Nelson LJ, Laserson KF, Holtz TH, Finlay A, Castro KG, Weyer K. HIV Infection and Multidrug-Resistant Tuberculosis – The Perfect Storm. The Journal of Infectious Diseases. 2007;196:S86–S107. - PubMed
-
- Multidrug and extensively drug-resistant TB (M/XDR-TB) Geneva, Switzerland: WHO global report on surveillance and response, World Health Organization; 2010. [Figure 4 from page 14 of the report is adopted as Figure 1a with permission from WHO]
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
