

Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype
- PMID: 22624038
- PMCID: PMC3356313
- DOI: 10.1371/journal.pone.0037483
Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype
Abstract
Background: Because chronic obstructive pulmonary disease (COPD) is a heterogeneous condition, the identification of specific clinical phenotypes is key to developing more effective therapies. To explore if the persistence of systemic inflammation is associated with poor clinical outcomes in COPD we assessed patients recruited to the well-characterized ECLIPSE cohort (NCT00292552).
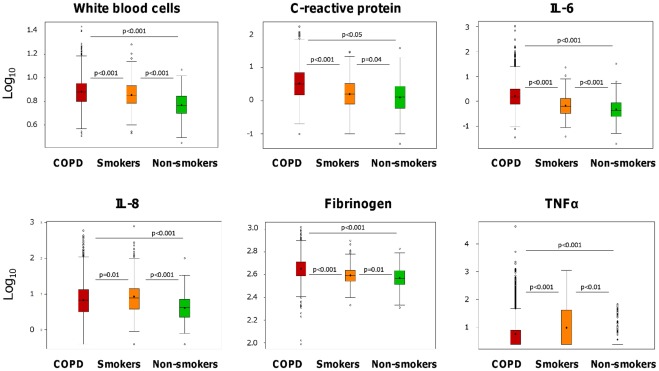
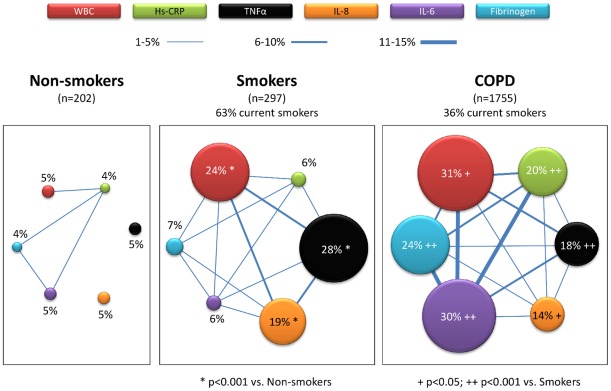
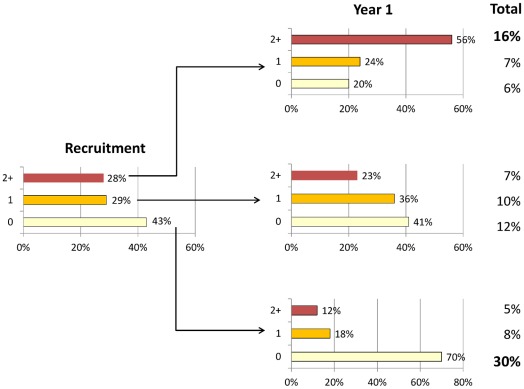
Methods and findings: Six inflammatory biomarkers in peripheral blood (white blood cells (WBC) count and CRP, IL-6, IL-8, fibrinogen and TNF-α levels) were quantified in 1,755 COPD patients, 297 smokers with normal spirometry and 202 non-smoker controls that were followed-up for three years. We found that, at baseline, 30% of COPD patients did not show evidence of systemic inflammation whereas 16% had persistent systemic inflammation. Even though pulmonary abnormalities were similar in these two groups, persistently inflamed patients during follow-up had significantly increased all-cause mortality (13% vs. 2%, p<0.001) and exacerbation frequency (1.5 (1.5) vs. 0.9 (1.1) per year, p<0.001) compared to non-inflamed ones. As a descriptive study our results show associations but do not prove causality. Besides this, the inflammatory response is complex and we studied only a limited panel of biomarkers, albeit they are those investigated by the majority of previous studies and are often and easily measured in clinical practice.
Conclusions: Overall, these results identify a novel systemic inflammatory COPD phenotype that may be the target of specific research and treatment.
Conflict of interest statement
Figures
References
-
- Rosenbaum L, Lamas D. New England Journal of Medicine; 2011. Facing a “Slow-Motion Disaster” - The UN Meeting on Noncommunicable Diseases. - PubMed
-
- Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370:765–773. - PubMed
-
- Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370:741–750. - PubMed
-
- Lopez AD, Murray CC. The global burden of disease, 1990–2020. Nat Med. 1998;4:1241–1243. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
