

Challenges of making a diagnosis in the outpatient setting: a multi-site survey of primary care physicians
- PMID: 22626738
- PMCID: PMC3680371
- DOI: 10.1136/bmjqs-2011-000541
Challenges of making a diagnosis in the outpatient setting: a multi-site survey of primary care physicians
Abstract
Background: Although misdiagnosis in the outpatient setting leads to significant patient harm and wasted resources, it is not well studied. The authors surveyed primary care physicians (PCPs) about barriers to timely diagnosis in the outpatient setting and assessed their perceptions of diagnostic difficulty.
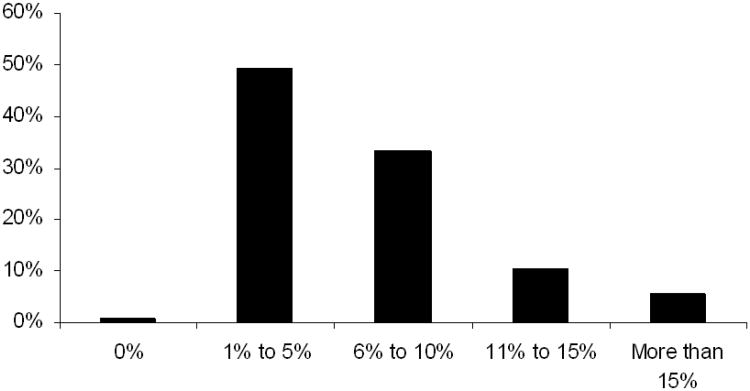
Methods: Surveys of PCPs practicing in an integrated health system across 10 geographically dispersed states in 2005. The survey elicited information on key cognitive failures (including in clinical knowledge or judgement) for a specific case, and solicited strategies for reducing diagnostic delays. Content analysis was used to categorise cognitive failures and strategies for improvement. The authors examined the extent and predictors of diagnostic difficulty, defined as reporting >5% patients difficult to diagnose.
Results: Of 1817 physicians surveyed, 1054 (58%) responded; 848 (80%) respondents primarily practiced in outpatient settings and had an assigned patient panel (inclusion sample). Inadequate knowledge (19.9%) was the most commonly reported cognitive factor. Half reported >5% of their patients were difficult to diagnose; more experienced physicians reported less diagnostic difficulty. In adjusted analyses, problems with information processing (information availability and time to review it) and the referral process were associated with greater diagnostic difficulty. Strategies for improvement most commonly involved workload issues (panel size, non-visit tasks).
Conclusions: PCPs report a variety of reasons for diagnostic difficulties in primary care practice. In this study, knowledge gaps appear to be a prominent concern. Interventions that address these gaps as well as practice level issues such as time to process diagnostic information and better subspecialty input may reduce diagnostic difficulties in primary care.
Conflict of interest statement
Competing Interests Statement: Authors report no competing interests
Figures
References
-
- Bishop TF, Ryan AM, Casalino LP. Paid malpractice claims for adverse events in inpatient and outpatient settings. Jama. 2011;305:2427–31. - PubMed
-
- Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med. 1991;324:377–84. - PubMed
-
- Thomas EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000;38:261–71. - PubMed
-
- Schiff GD, Hasan O, Kim S, et al. Diagnostic error in medicine: analysis of 583 physician-reported errors. Arch Intern Med. 2009;169:1881–7. - PubMed
-
- Graber M. Diagnostic errors in medicine: a case of neglect. Jt Comm J Qual Patient Saf. 2005;31:106–13. - PubMed