

Surgical repair of ventricular septal defect after myocardial infarction: outcomes from the Society of Thoracic Surgeons National Database
- PMID: 22626761
- PMCID: PMC3608099
- DOI: 10.1016/j.athoracsur.2012.04.020
Surgical repair of ventricular septal defect after myocardial infarction: outcomes from the Society of Thoracic Surgeons National Database
Abstract
Background: The development of a ventricular septal defect (VSD) after myocardial infarction (MI) is an uncommon but highly lethal complication. We examined The Society of Thoracic Surgeons database to characterize patients undergoing surgical repair of post-MI VSD and to identify risk factors for poor outcomes.
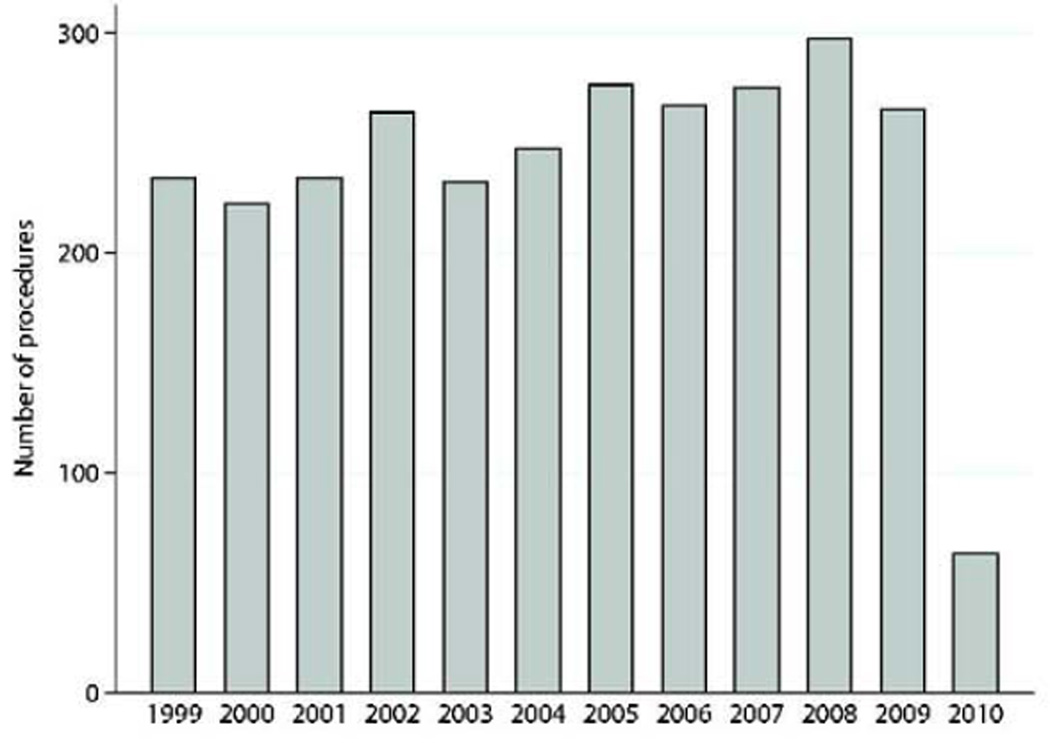
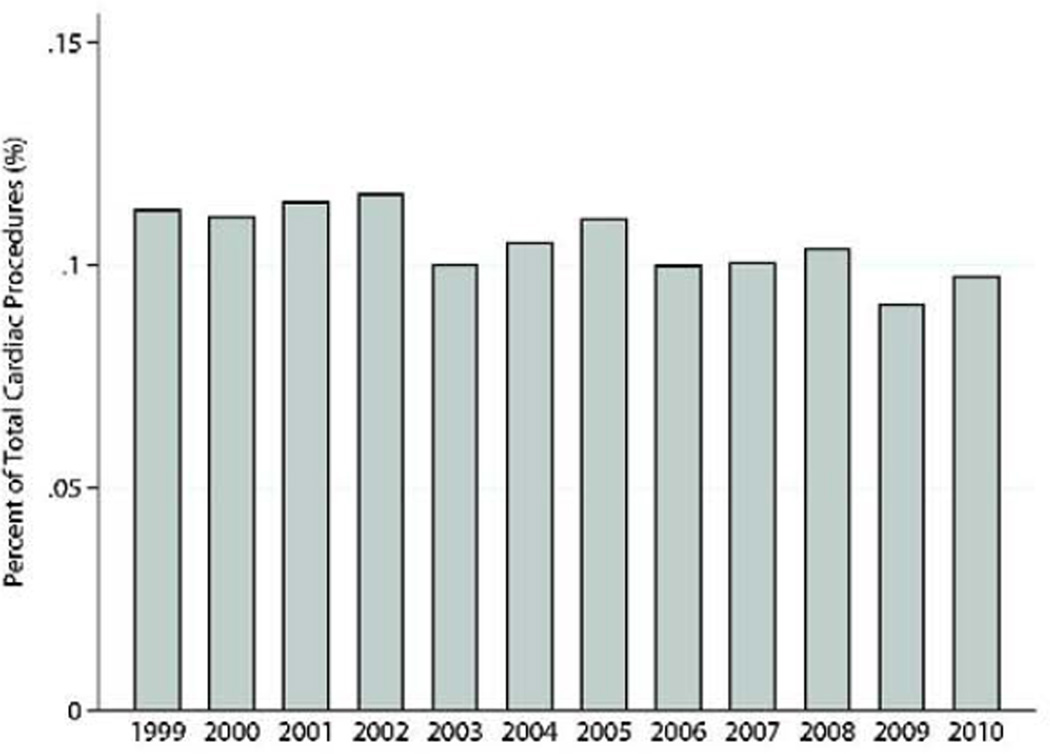
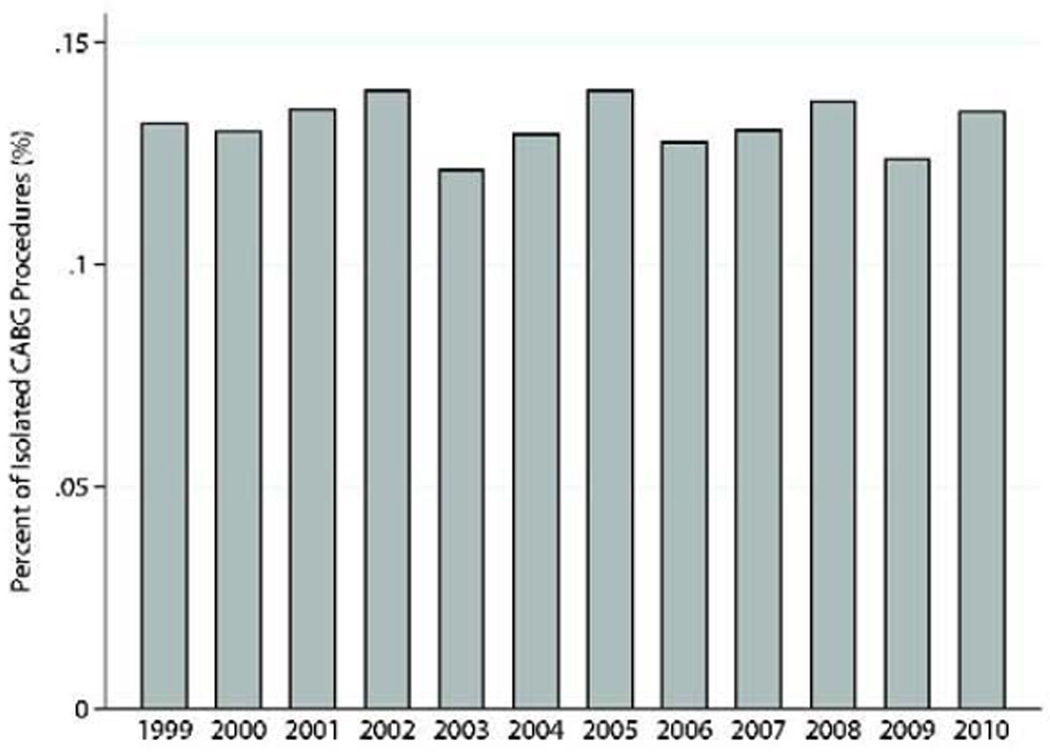
Methods: This was a retrospective review of The Society of Thoracic Surgeons database to identify adults (aged≥18 years) who underwent post-MI VSD repair between 1999 and 2010. Patients with congenital heart disease were excluded. The primary outcome was operative death. The covariates in the current The Society of Thoracic Surgeons model for predicted coronary artery bypass grafting operative death were incorporated in a logistic regression model in this cohort.
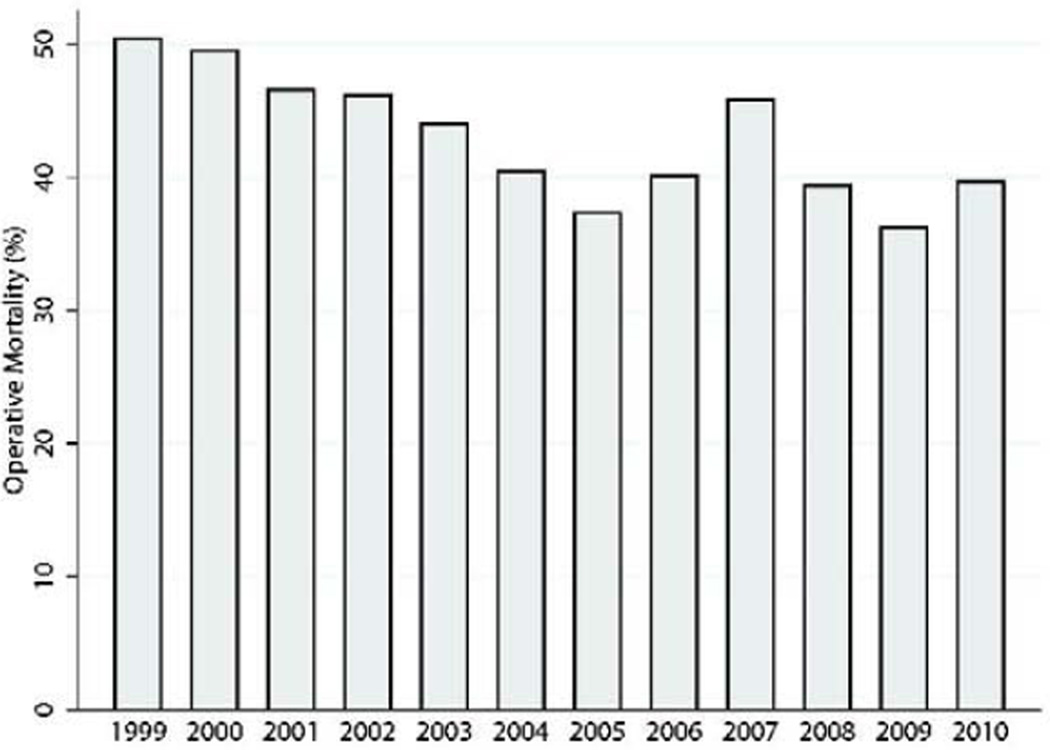
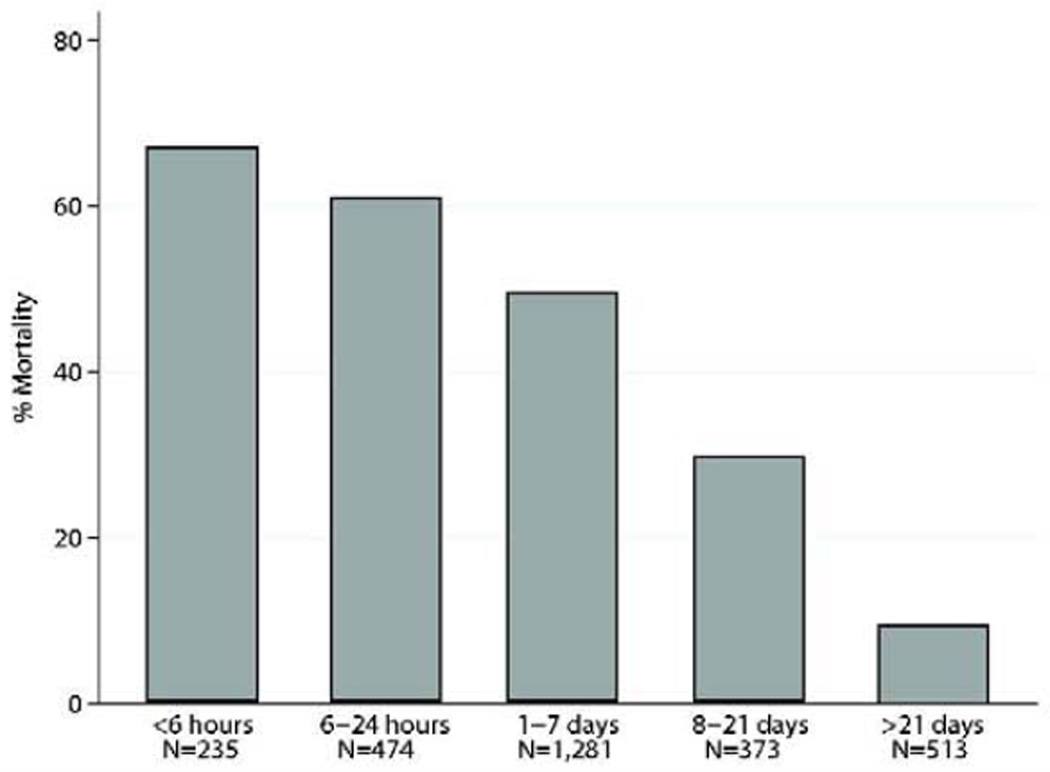
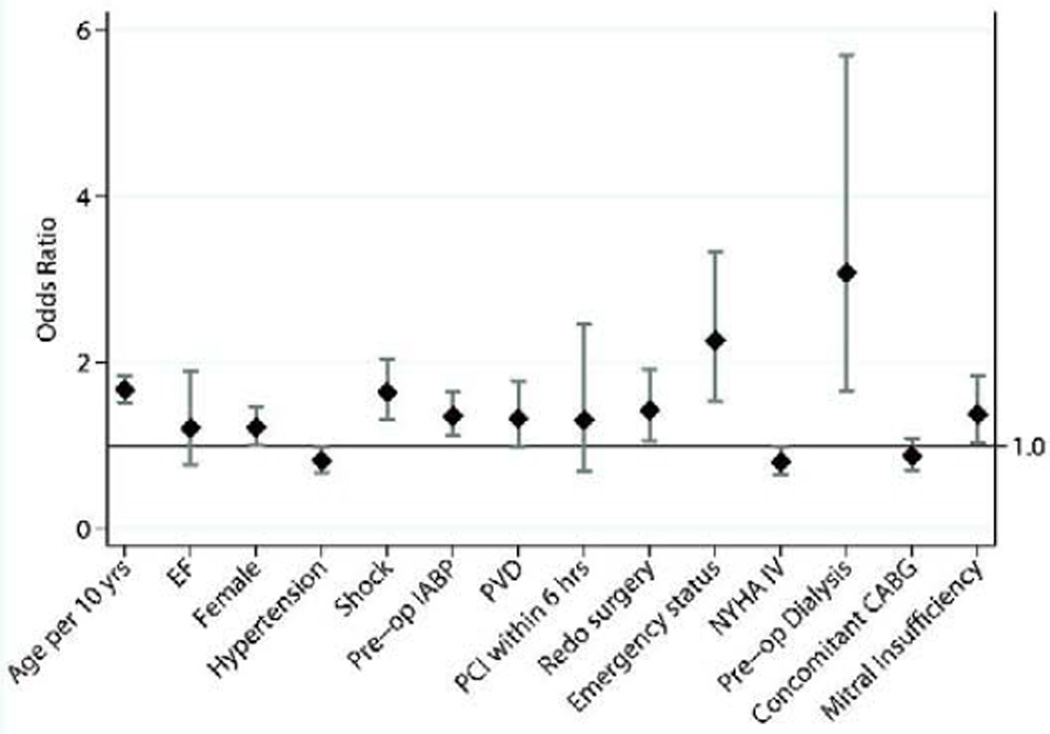
Results: The study included 2,876 patients (1,624 men [56.5%]), who were a mean age of 68±11 years. Of these, 215 (7.5%) had prior coronary artery bypass grafting operations, 950 (33%) had prior percutaneous intervention, and 1,869 (65.0%) were supported preoperatively with an intraaortic balloon pump. Surgical status was urgent in 1,007 (35.0%) and emergencies in 1,430 (49.7%). Concomitant coronary artery bypass grafting was performed in 1,837 (63.9%). Operative mortality was 54.1% (1,077 of 1,990) if repair was within 7 days from MI and 18.4% (158 of 856) if more than 7 days from MI. Multivariable analysis identified several factors associated with increased odds of operative death.
Conclusions: In the largest study to date to examine post-MI VSD repair, ventricular septal rupture remains a devastating complication. As alternative therapies emerge to treat this condition, these results will serve as a benchmark for future comparisons.
Copyright © 2012 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Crenshaw BS, Granger CB, Birnbaum Y, et al. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators. Circulation. 2000;101(1):27–32. - PubMed
-
- Jeppsson A, Liden H, Johnsson P, Hartford M, Radegran K. Surgical repair of post infarction ventricular septal defects: a national experience. Eur J Cardiothorac Surg. 2005;27(2):216–221. - PubMed
-
- David TE, Armstrong S. Surgical repair of postinfarction ventricular septal defect by infarct exclusion. Semin Thorac Cardiovasc Surg. 1998;10(2):105–110. - PubMed
-
- Muehrcke DD, Daggett WM, Jr, Buckley MJ, Akins CW, Hilgenberg AD, Austen WG. Postinfarct ventricular septal defect repair: effect of coronary artery bypass grafting. Ann Thorac Surg. 1992;54(5):876–882. discussion 82–3. - PubMed
-
- Labrousse L, Choukroun E, Chevalier JM, et al. Surgery for post infarction ventricular septal defect (VSD): risk factors for hospital death and long term results. Eur J Cardiothorac Surg. 2002;21(4):725–731. discussion 31–2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
