

Preoperative cognitive dysfunction is related to adverse postoperative outcomes in the elderly
- PMID: 22626912
- PMCID: PMC3383613
- DOI: 10.1016/j.jamcollsurg.2012.02.007
Preoperative cognitive dysfunction is related to adverse postoperative outcomes in the elderly
Abstract
Background: Preoperative risk stratification is commonly performed by assessing end-organ function (such as cardiac and pulmonary) to define postoperative risk. Little is known about impaired preoperative cognition and outcomes. The purpose of this study was to evaluate the impact of baseline impaired cognition on postoperative outcomes in geriatric surgery patients.
Study design: Subjects 65 years and older undergoing a planned elective operation requiring postoperative ICU admission were recruited prospectively. Preoperative baseline cognition was assessed using the validated Mini-Cog test. Impaired cognition was defined as a Mini-Cog score of ≤ 3. Delirium was assessed using the Confusion Assessment Method-ICU by a trained research team. Adverse outcomes were defined using the Veterans Affairs Surgical Quality Improvement Program definitions.
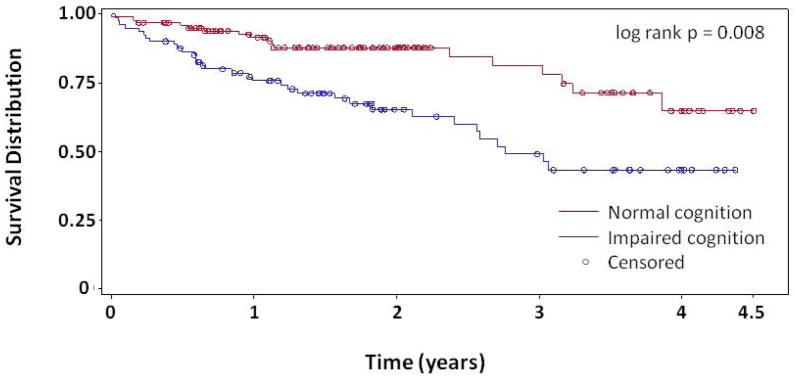
Results: One hundred and eighty-six subjects were included, with a mean age of 73 ± 6 years. Eighty-two subjects (44%) had baseline impaired cognition. The impaired cognition group had the following unadjusted outcomes: increased incidence of 1 or more postoperative complications (41% vs 24%; p = 0.011), higher incidence of delirium (78% vs 37%; p < 0.001), longer hospital stays (15 ± 14 vs 9 ± 9 days; p = 0.001), higher rate of discharge institutionalization (42% vs 18%; p = 0.001), and higher 6-month mortality (13% vs 5%; p = 0.040). Adjusting for potential confounders determined by univariate analysis, logistic regression found impaired cognition was still associated with the occurrence of 1 or more postoperative complications (odds ratio = 2.401; 95% CI, 1.185-4.865; p = 0.015). Kaplan-Meier survival analysis revealed higher mortality in the impaired cognition group (log-rank p = 0.008).
Conclusions: Baseline cognitive impairment in older adults undergoing major elective operations is related to adverse postoperative outcomes including increased complications, length of stay, and long-term mortality. Improved understanding of baseline cognition and surgical outcomes can aid surgical decision making in older adults.
Published by Elsevier Inc.
References
-
- Laine C, Williams SV, Wilson JF. In the clinic. Preoperative evaluation. Ann Intern Med. 2009;151:ITC1-15. quiz ITC16. - PubMed
-
- Fleisher LA, Beckman JA, Brown KA, et al. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery. J Am Coll Cardiol. 2009;54:e13–e118. - PubMed
-
- Calderini E, Adrario E, Petrini F, et al. Indications to chest radiograph in preoperative adult assessment: recommendations of the SIAARTI-SIRM commission. Minerva Anestesiol. 2004;70:443–451. - PubMed
-
- Schneider PD. Preoperative assessment of liver function. Surg Clin North Am. 2004;84:355–373. - PubMed
-
- Michota FA., Jr The preoperative evaluation and use of laboratory testing. Cleve Clin J Med. 2006;73 (Suppl 1):S4–7. - PubMed
