

Case Reports
doi: 10.1038/ijos.2012.23.
Long-term follow-ups of revascularized immature necrotic teeth: three case reports
Affiliations
- PMID: 22627612
- PMCID: PMC3421481
- DOI: 10.1038/ijos.2012.23
Item in Clipboard
Case Reports
Long-term follow-ups of revascularized immature necrotic teeth: three case reports
Int J Oral Sci.
2012 Jun.
Abstract
Revascularization of immature necrotic teeth is a reliable treatment alternative to conventional apexogenesis or apexification. In case 1, a 12-year-old boy had his necrotic, immature mandibular left second premolar treated with a revascularization technique. At a24-month follow-up, periapical radiolucency had disappeared and thickening of the root wall was observed. In cases 2 and 3, a10-year-old boy had his necrotic, immature, bilateral mandibular second premolars treated with the same modality. At 48-month(in case 2) and 42-month (in case 3) follow-ups, loss of periapical radiolucencies and increases in the root wall thickness were also observed.
Figures
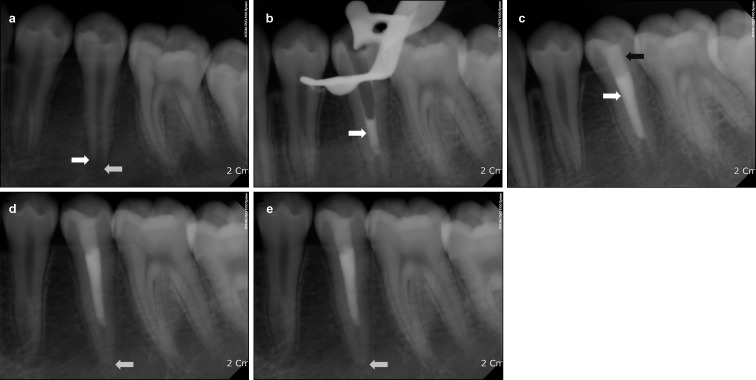
Periapical radiographs in case 1. (a) Pre-treatment periapical radiograph of the mandibular left second premolar. Note the periapical radiolucency and root immaturity (white arrows). (b) Periapical radiograph obtained immediately after placement of MTA into the root canal (white arrow). (c) Periapical radiograph obtained after gutta-percha (white arrow) obturation and composite resin restoration (black arrow). (d) Periapical radiograph obtained at the 6-week follow-up. Note the diminished periapical radiolucency (white arrow). (e) Periapical radiograph obtained at the 24-month follow-up. The root wall thickness has increased (white arrow) and apical closure is complete. MTA, mineral trioxide aggregate.
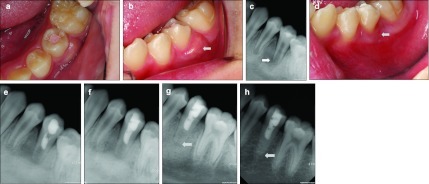
Intraoral photographs and periapical radiographs in case 2. (a) Pre-treatment occlusal photograph of the mandibular left second premolar. (b) Pre-treatment intraoral photograph of the tooth. Gingival swelling is evident on the buccal side (white arrow). (c) Pre-treatment periapical radiograph of the tooth. Periapical radiolucency with root immaturity is evident (white arrow). (d) Intraoral photograph obtained 2 weeks later. Buccal gingival swelling has disappeared (white arrow). (e) Periapical radiograph obtained immediately after placement of MTA into the root canal. (f) Periapical radiograph obtained after gutta-percha obturation and composite resin restoration. (g) Periapical radiograph obtained at the 2-month follow-up. Periapical radiolucency has decreased and the root wall has thickened (white arrow). (h) Periapical radiograph obtained at the 48-month follow-up. Thickening of the root wall is evident and periapical radiolucency has disappeared completely (white arrow). MTA, mineral trioxide aggregate.
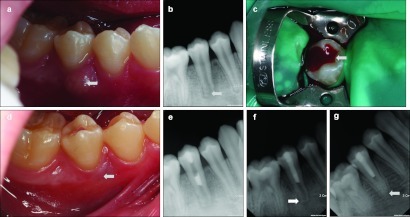
Intraoral photographs and periapical radiographs in case 3. (a) Pre-treatment intraoral photograph of the mandibular right second premolar. Gingival swelling on the buccal side is evident (white arrow). (b) Pre-treatment periapical radiograph of the tooth. Note the periapical radiolucency with thin root walls (white arrow). (c) Intraoral photograph obtained after access cavity preparation. Note the bloody purulent discharge (white arrow). (d) Intraoral photograph obtained 1 week later. Complete reduction of gingival swelling is evident (white arrow). (e) Periapical radiograph obtained immediately after placement of MTA into the root canal. (f) Periapical radiograph obtained at the 2-month follow-up. Periapical radiolucency has decreased (white arrow). (g) Periapical radiograph obtained at the 42-month follow-up. Thickness of the root wall has increased and the periapical radiolucency has disappeared completely (white arrow). MTA, mineral trioxide aggregate.
Similar articles
-
Regenerative endodontic treatment (revascularization) of immature necrotic molars medicated with calcium hydroxide: a case series.J Endod. 2011 Sep;37(9):1327-30. doi: 10.1016/j.joen.2011.05.033. Epub 2011 Jul 13. J Endod. 2011. PMID: 21846559
-
Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures.Int Endod J. 2012 Mar;45(3):294-305. doi: 10.1111/j.1365-2591.2011.01978.x. Epub 2011 Nov 14. Int Endod J. 2012. PMID: 22077958
-
Outcome of Revascularization Procedure: A Retrospective Case Series.J Endod. 2016 Dec;42(12):1752-1759. doi: 10.1016/j.joen.2016.06.021. Epub 2016 Oct 7. J Endod. 2016. PMID: 27726882
-
Revascularization: a treatment for permanent teeth with necrotic pulp and incomplete root development.J Endod. 2013 Mar;39(3):319-26. doi: 10.1016/j.joen.2012.11.014. Epub 2013 Jan 16. J Endod. 2013. PMID: 23402501 Review.
-
Recommendations for using regenerative endodontic procedures in permanent immature traumatized teeth.Dent Traumatol. 2012 Feb;28(1):33-41. doi: 10.1111/j.1600-9657.2011.01044.x. Epub 2011 Jul 27. Dent Traumatol. 2012. PMID: 21794081 Review.
Cited by
-
Regenerative endodontic procedure using Emdogain: a case series.J Med Case Rep. 2025 May 2;19(1):205. doi: 10.1186/s13256-025-05199-x. J Med Case Rep. 2025. PMID: 40317062 Free PMC article.
-
Regenerative endodontic treatment of dens in dente in maxillary lateral incisor with immature root: a case report.Hua Xi Kou Qiang Yi Xue Za Zhi. 2022 Dec 1;40(6):716-720. doi: 10.7518/hxkq.2022.06.014. Hua Xi Kou Qiang Yi Xue Za Zhi. 2022. PMID: 36416326 Free PMC article. Chinese, English.
-
Revascularization Revisited with Modified Triple Antibiotic Paste and NeoPutty MTA®.J Pharm Bioallied Sci. 2024 Apr;16(Suppl 2):S1871-S1874. doi: 10.4103/jpbs.jpbs_1212_23. Epub 2024 Apr 16. J Pharm Bioallied Sci. 2024. PMID: 38882759 Free PMC article.
-
Efficacy of Biodentine as an Apical Plug in Nonvital Permanent Teeth with Open Apices: An In Vitro Study.Biomed Res Int. 2015;2015:359275. doi: 10.1155/2015/359275. Epub 2015 Sep 7. Biomed Res Int. 2015. PMID: 26436090 Free PMC article.
-
Roles of Dental Mesenchymal Stem Cells in the Management of Immature Necrotic Permanent Teeth.Front Cell Dev Biol. 2021 May 19;9:666186. doi: 10.3389/fcell.2021.666186. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34095133 Free PMC article. Review.
References
-
- Cvek M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Endod Dent Traumatol. 1992;8 2:45–55. - PubMed
-
- Mente J, Hage N, Pfefferle T, et al. Mineral trioxide aggregate apical plugs in teeth with open apical foramina: a retrospective analysis of treatment outcome. J Endod. 2009;35 10:1354–1358. - PubMed
-
- Al Ansary MA, Day PF, Duggal MS, Brunton PA. Interventions for treating traumatized necrotic immature permanent anterior teeth: inducing a calcific barrier & root strengthening. Dent Traumatol. 2009;25 4:367–379. - PubMed
-
- Sheehy EC, Roberts GJ. Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: a review. Br Dent J. 1997;183 7:241–246. - PubMed
-
- Torabinejad M, Parirokh M. Mineral trioxide aggregate: a comprehensive literature review—Part II: Leakage and biocompatibility investigations. J Endod. 2010;36 2:190–202. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
