

Review
doi: 10.1038/nri3226.
Emerging concepts in haematopoietic cell transplantation
Affiliations
- PMID: 22627859
- PMCID: PMC4006975
- DOI: 10.1038/nri3226
Item in Clipboard
Review
Emerging concepts in haematopoietic cell transplantation
Nat Rev Immunol.
.
Abstract
Haematopoietic cell transplantation (HCT) is the most widely used form of cellular therapy. It is the only known cure for some haematological malignancies and has recently been used in additional clinical settings, such as allograft tolerance induction and treatment of autoimmune diseases. Recent advances have enabled HCT in a wider range of patients with improved outcomes. This Review summarizes the latest developments in this therapy, focusing on issues that will affect future advancement.
Figures
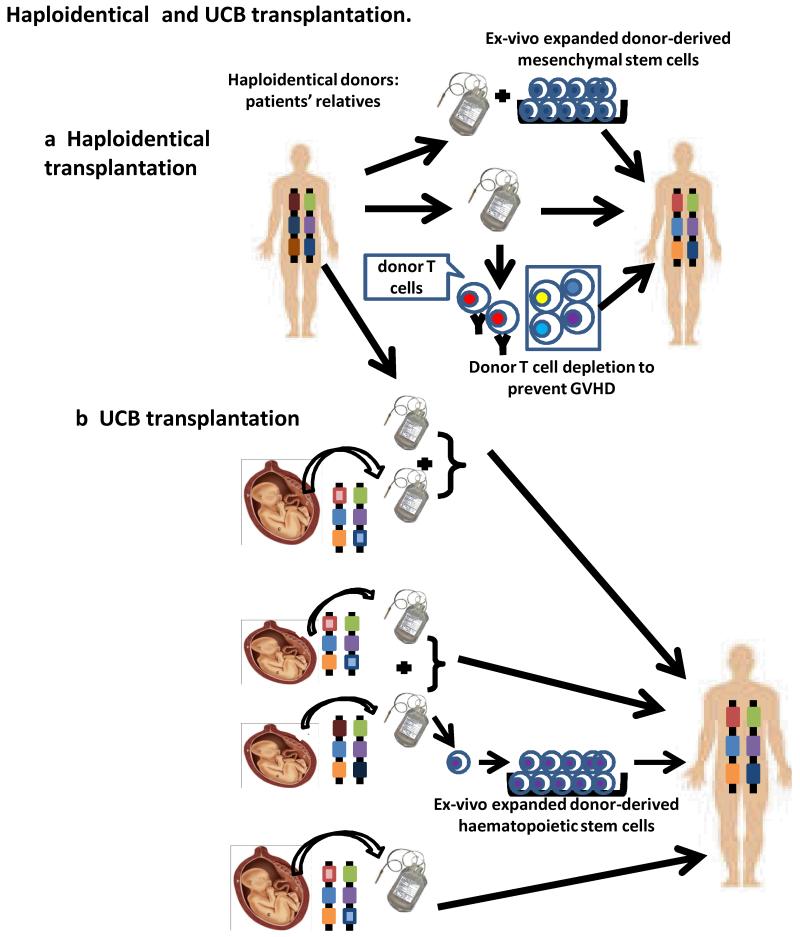
a| Haploidentical grafts can be derived from the patient’s parents, siblings or children (or other relatives). T celldepletion may be performed to prevent GVHD, or donor-derived ex-vivo expanded mesenchymal stem cells may be added to the grafts to enhance engraftment or prevent GVHD. b| Although a single unit of UCB graft can be used for HCT, the limited number of haematopoietic stem cells is often associated with delayed engraftment and immune reconstitution. Addition of a second unit of UCB, or ex-vivo expanded haematopoietic stem cells from another unit of UCB, or a haploidentical adult hematopoietic donor graft can enhance engraftment.
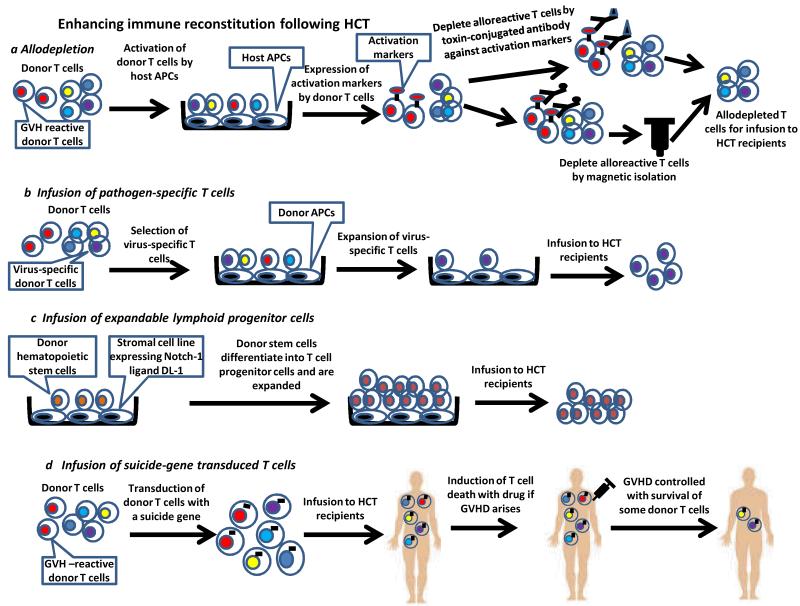
a|To generate allodepleted donor T cells for transfer, donor T cells are activated by host APCs followed by treatment with toxin-conjugated antibodies against activation markers or by antibody with magnetic separation. b|Pathogen-specific T cells must first be isolated and are then expanded ex vivo before infusion to HCT recipients. c|T progenitor cells can be generated in vitro by coculture of the donor haematopoietic stem cells with the stromal cell line expressing Delta-like-1 (DL-1), which is a ligand of Notch-1. Stem cells will differentiate into T progenitor cells and are expanded in number. The T progenitor cells are then infused to HCT recipients. d|To allow for control of GVHD induced by donor T cells given to enhance immune reconstitution of HCT recipients, donor T cells are first transduced with a suicide gene that enables the cells to be killed by exogenous agents interacting with the transduced gene product. The suicide gene-transduced donor T cells are infused to HCT recipients. When GVHD arises, the transduced donor T cells are induced to die so that GVHD can be controlled. A small number of transduced donor T cells will survive.
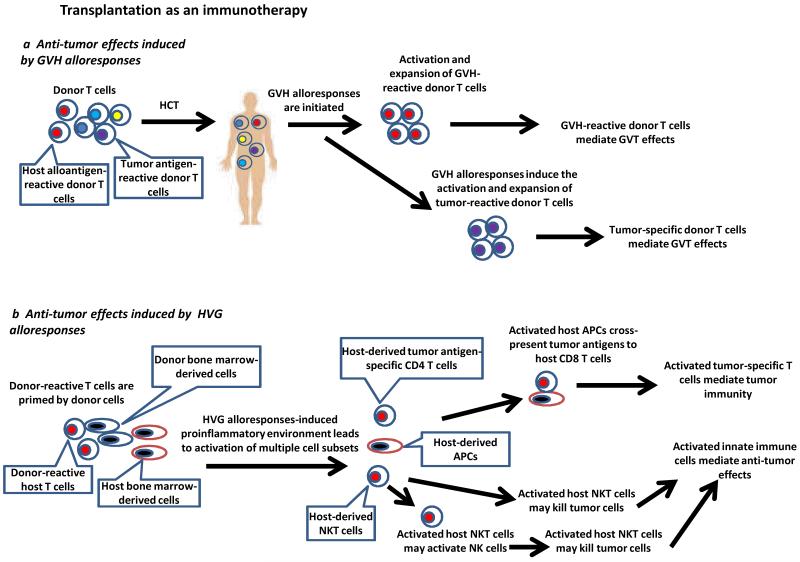
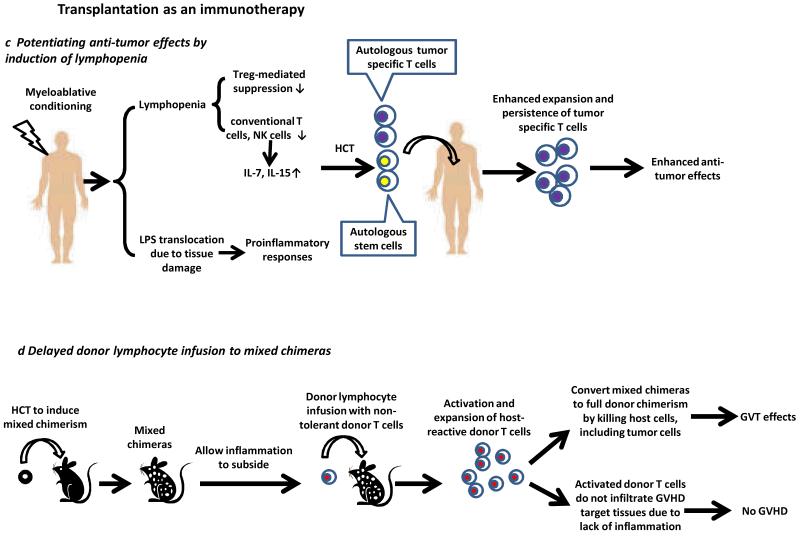
a|GVH-reactive T cells and tumor-specific donor T cells activated during GVH alloresponses may contribute to GVT effects. b| Immune activation due to HVG alloresponses leads to activation of multiple cell types. Activated NKT cells may facilitate the activation of host APCs, such as dendritic cells, and their interactions with tumor-specific CD4 T cells. This leads to enhanced cross-presentation of tumor antigens and activation of tumor antigen-specific host CD8 T cells that kill tumor cells. The activated NKT cells may exert tumorocidal activities or activate NK cells to mediate anti-tumor effects. c|In patients receiving myeloablative conditioning to induce lymphopenia, reduced Treg-mediated suppression, increased availability of cytokines and translocation of LPS collectively lead to enhanced anti-tumor effects mediated by tumor-specific T cells. Autologous HCT is required for rescue of hematologic failure. d|GVHD and GVT effects can be separated by delayed administration of DLI to established mixed chimeras. Host-reactive T cells are activated and eliminate all host hematopoietic cells, including tumor cells, thus mediating GVT effects. The lack of tissue inflammation in established mixed chimeras receiving these DLI prevents GVH-reactive donor T cells from infiltrating the GVHD target tissues.
a|GVH-reactive T cells and tumor-specific donor T cells activated during GVH alloresponses may contribute to GVT effects. b| Immune activation due to HVG alloresponses leads to activation of multiple cell types. Activated NKT cells may facilitate the activation of host APCs, such as dendritic cells, and their interactions with tumor-specific CD4 T cells. This leads to enhanced cross-presentation of tumor antigens and activation of tumor antigen-specific host CD8 T cells that kill tumor cells. The activated NKT cells may exert tumorocidal activities or activate NK cells to mediate anti-tumor effects. c|In patients receiving myeloablative conditioning to induce lymphopenia, reduced Treg-mediated suppression, increased availability of cytokines and translocation of LPS collectively lead to enhanced anti-tumor effects mediated by tumor-specific T cells. Autologous HCT is required for rescue of hematologic failure. d|GVHD and GVT effects can be separated by delayed administration of DLI to established mixed chimeras. Host-reactive T cells are activated and eliminate all host hematopoietic cells, including tumor cells, thus mediating GVT effects. The lack of tissue inflammation in established mixed chimeras receiving these DLI prevents GVH-reactive donor T cells from infiltrating the GVHD target tissues.
References
-
- Barker JN, et al. Transplantation of 2 partially HLA-matched umbilical cord blood units to enhance engraftment in adults with hematologic malignancy. Blood. 2005;105:1343–1347. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
