

Pharmacokinetics and safety of fluconazole in young infants supported with extracorporeal membrane oxygenation
- PMID: 22627870
- PMCID: PMC3444624
- DOI: 10.1097/INF.0b013e31825d3091
Pharmacokinetics and safety of fluconazole in young infants supported with extracorporeal membrane oxygenation
Abstract
Background: Candida infections are a leading cause of infectious disease-related death in infants supported with extracorporeal membrane oxygenation (ECMO). The ECMO circuit can alter drug pharmacokinetics; thus, standard fluconazole dosing in children on ECMO may result in suboptimal drug exposure. This study determined the pharmacokinetics of fluconazole in infants on ECMO.
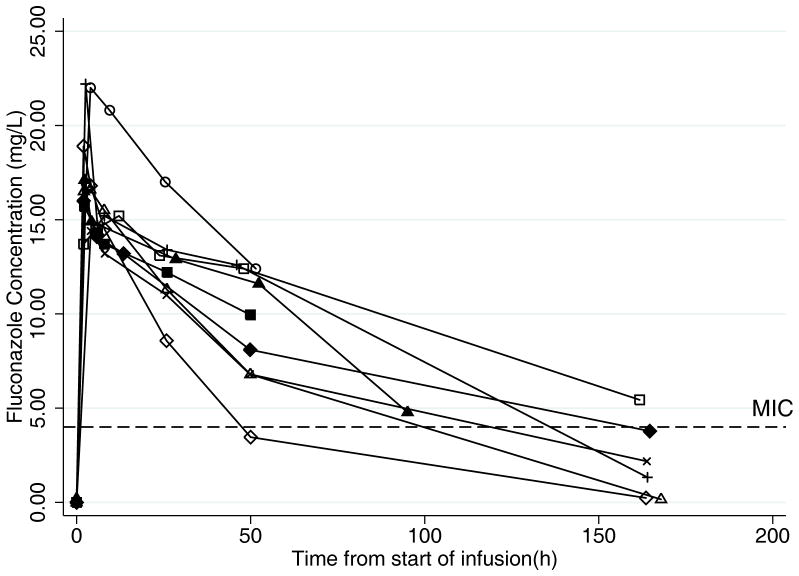
Methods: Infants <120 days of age received either intravenous fluconazole prophylaxis (25 mg/kg once a week) or treatment (12 mg/kg daily) while on ECMO. Paired plasma samples were collected preoxygenator and postoxygenator around doses 1 and 2 to calculate pharmacokinetic indices and describe oxygenator extraction. A 1-compartment model was fit to the data using nonlinear regression. Surrogate pharmacodynamic targets for efficacy were evaluated.
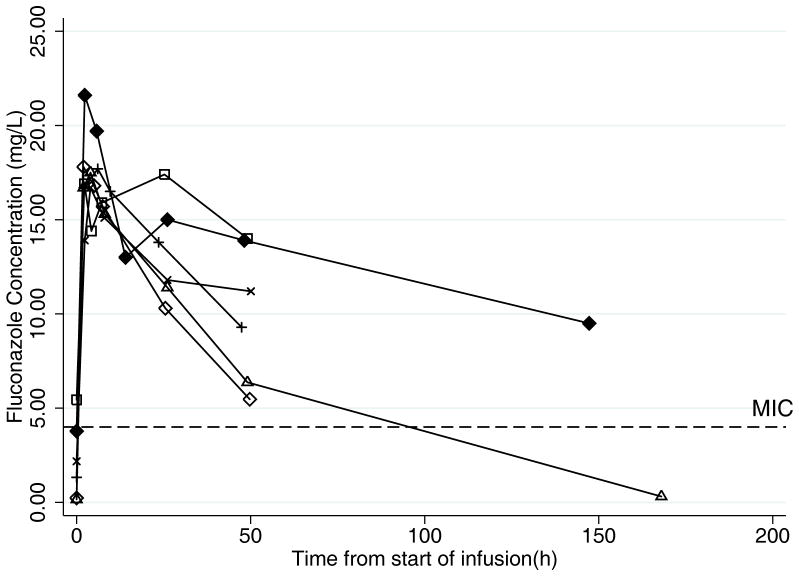
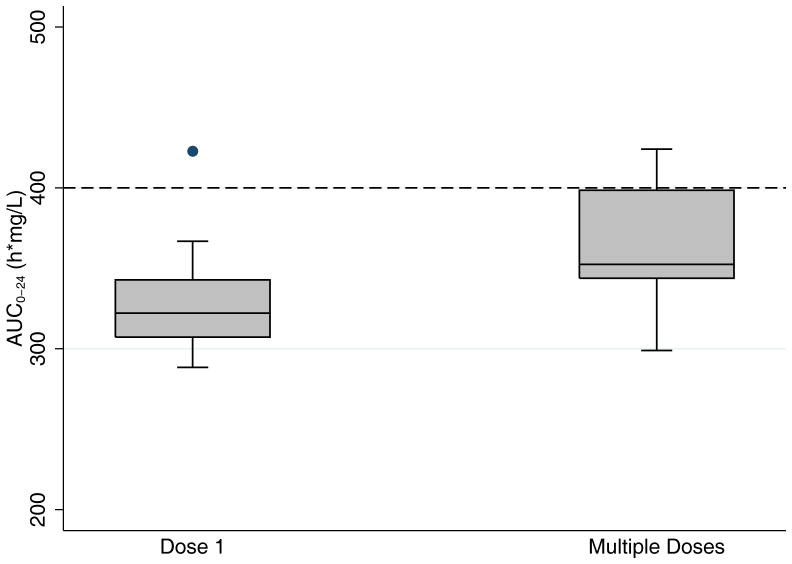
Results: Ten infants were enrolled. After dose 1 (n = 9), the median clearance was 17 mL/kg/h, the median volume of distribution was 1.5 L/kg and the median exposure in the first 24 hours (area under the curve from 0 to 24 hours) was 322 h × mg/L. After multiple doses (n = 7), the median clearance was 22 mL/kg/h, the median volume of distribution was 1.9 L/kg and the area under the curve from 0 to 24 hours was 352 h × mg/L. After dose 1, 78% of infants achieved the prophylaxis target, whereas only 11% achieved the therapeutic target. Oxygenator extraction of fluconazole was minimal (-2.0%, standard deviation 15.0), and extraction was not correlated with age of the ECMO circuit (ρ= -0.05). There were no adverse events related to fluconazole.
Conclusions: Infants on ECMO had higher volume of distribution but similar clearance when compared with historical controls not on ECMO. In infants on ECMO, a fluconazole dose of 25 mg/kg weekly provides adequate exposure for prophylaxis against Candida infections. However, higher doses may be needed for treatment.
Figures
References
-
- Extracorporeal Life Support Organization (ELSO) Extracorporeal Life Support Registry Report: International Summary. Ann Arbor, MI: ELSO; 2010.
-
- Bizzarro MJ, Conrad SA, Kaufman DA, Rycus P Extracorporeal Life Support Organization Task Force on Infections, Extracorporeal Membrane Oxygenation. Infections acquired during extracorporeal membrane oxygenation in neonates, children, and adults. Pediatr Crit Care Med. 2011;12:277–281. - PubMed
-
- Gardner AH, Prodhan P, Stovall SH, et al. Fungal infections and antifungal prophylaxis in pediatric cardiac extracorporeal life support. J Thorac Cardiovasc Surg. 2011 Dec 15; [Epub ahead of print] - PubMed
-
- Eppes SC, Troutman JL, Gutman LT. Outcome of treatment of candidemia in children whose central catheters were removed or retained. Pediatr Infect Dis J. 1989;8:99–104. - PubMed
-
- Veinstein A, Debouverie O, Grégoire N, et al. Lack of effect of extracorporeal membrane oxygenation on tigecycline pharmacokinetics. J Antimicrob Chemother. 2011 Dec 29; [Epub ahead of print] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN267200700051C/HD/NICHD NIH HHS/United States
- T32 HD043029/HD/NICHD NIH HHS/United States
- R01 GM041935/GM/NIGMS NIH HHS/United States
- R01 HD057956/HD/NICHD NIH HHS/United States
- 1R01HD057956-02/HD/NICHD NIH HHS/United States
- 5T32HD043029-09/HD/NICHD NIH HHS/United States
- K23 HD064814/HD/NICHD NIH HHS/United States
- 1R18AE000028-01/AE/ASPE HHS/United States
- 1K24HD058735-01/HD/NICHD NIH HHS/United States
- R01 FD003519/FD/FDA HHS/United States
- 1R01FD003519-01/FD/FDA HHS/United States
- 1T32GM086330-01A1/GM/NIGMS NIH HHS/United States
- K23 HD060040/HD/NICHD NIH HHS/United States
- K24 HD058735/HD/NICHD NIH HHS/United States
- HHSN275201000002C/HD/NICHD NIH HHS/United States
- 1K23HD064814-01/HD/NICHD NIH HHS/United States
- U10 HD045962/HD/NICHD NIH HHS/United States
- 3R01GM41935-19/GM/NIGMS NIH HHS/United States
- 1K23HD060040-01/HD/NICHD NIH HHS/United States
- T32 GM086330/GM/NIGMS NIH HHS/United States
- 1U10-HD45962-06/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
