

Management of cartilage defects in the shoulder
- PMID: 22628177
- PMCID: PMC3535081
- DOI: 10.1007/s12178-012-9131-1
Management of cartilage defects in the shoulder
Abstract
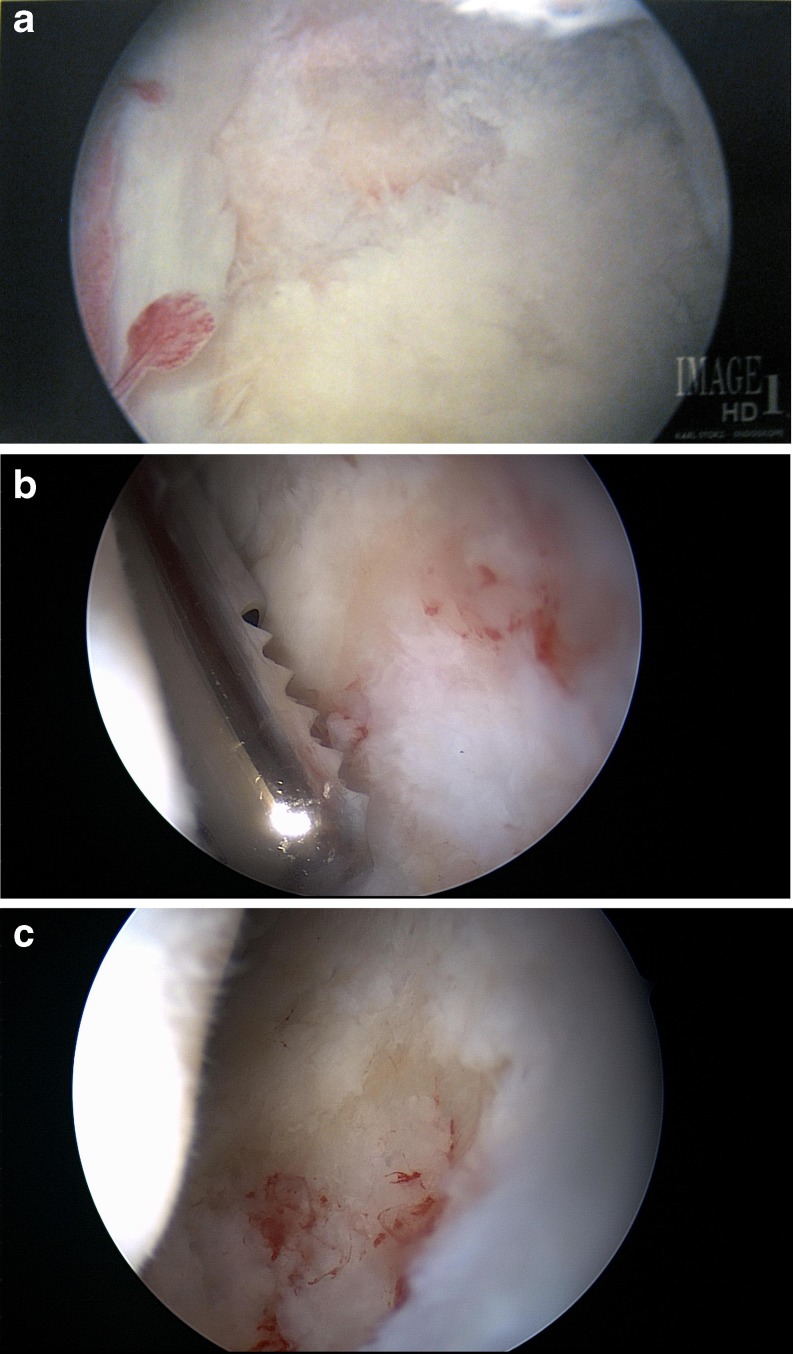
Articular cartilage lesions of the glenohumeral joint are an especially difficult clinical problem to manage, particularly in the younger, more active patient. Left untreated, these lesions may progress in the long-term, leading to further pain and disability. While shoulder arthroplasty remains a viable option in older patients with glenohumeral arthritis, concerns over component longevity and loosening in younger patients make it less attractive in that age group. Arthroscopic joint debridement with loose body removal, often with capsular release, has been successful in select, more sedentary patients. More recent techniques, including autologous chondrocyte implantation (ACI), osteochondral grafting (allograft versus autograft), interpositional arthroplasty, and microfracture surgery, have been evaluated for use in the shoulder. These procedures have experienced success in weight bearing joints, including the knee and ankle. Despite the good clinical results in the shoulder with short-term follow-up reported in some small series, the treatment of chondral injuries in the glenohumeral joint remains a challenging problem.
Figures
References
-
- Provencher MT, Barker JU, Strauss EJ, et al. Glenohumeral arthritis in the young adult. Instr Course Lect. 2011;60:137–53. - PubMed
LinkOut - more resources
Full Text Sources
