

Medical marijuana: clearing away the smoke
- PMID: 22629287
- PMCID: PMC3358713
- DOI: 10.2174/1874205X01206010018
Medical marijuana: clearing away the smoke
Abstract
Recent advances in understanding of the mode of action of tetrahydrocannabinol and related cannabinoid in-gredients of marijuana, plus the accumulating anecdotal reports on potential medical benefits have spurred increasing re-search into possible medicinal uses of cannabis. Recent clinical trials with smoked and vaporized marijuana, as well as other botanical extracts indicate the likelihood that the cannabinoids can be useful in the management of neuropathic pain, spasticity due to multiple sclerosis, and possibly other indications. As with all medications, benefits and risks need to be weighed in recommending cannabis to patients. We present an algorithm that may be useful to physicians in determining whether cannabis might be recommended as a treatment in jurisdictions where such use is permitted.
Keywords: Cannabis; chronic pain; pain..
Figures
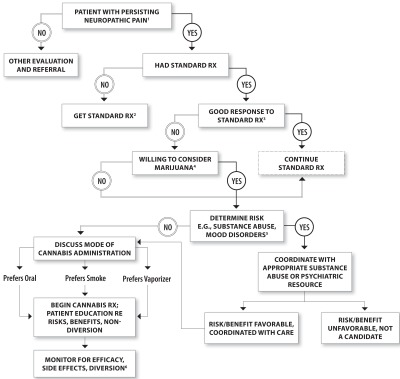
Daily or almost daily pain with typical neuropathic characteristics for at least 3 months; affects life quality.
Standard Rx = e.g., antidepressants, anticonvulsants; opioids; nonsteroidal anti-inflammatory drugs.
For example, at least 30% reduction in pain intensity.
Consider past experience, possible past history of side effects; willingness to smoke.
Determine history of substance abuse. If yes, or at “high risk” aberrant for drug behavior; proceed with close observation; possibly coor-dinate with substance abuse treatment program.
Efficacy = at least 30% reduction in pain intensity.
References
-
- Huestis MA. Pharmacokinetics and metabolism of the plant cannabinoids, delta9-tetrahydrocannabinol, cannabidiol and cannabinol. Handb Exp Pharmacol. 2005;(168):657–90. - PubMed
-
- Abrams DI, Jay CA, Shade SB, et al. Cannabis in painful HIV-associated sensory neuropathy: a randomized placebo-controlled trial. Neurology. 2007;68(7):515–21. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials