

Feasibility of prehospital teleconsultation in acute stroke--a pilot study in clinical routine
- PMID: 22629331
- PMCID: PMC3356340
- DOI: 10.1371/journal.pone.0036796
Feasibility of prehospital teleconsultation in acute stroke--a pilot study in clinical routine
Abstract
Background: Inter-hospital teleconsultation improves stroke care. To transfer this concept into the emergency medical service (EMS), the feasibility and effects of prehospital teleconsultation were investigated.
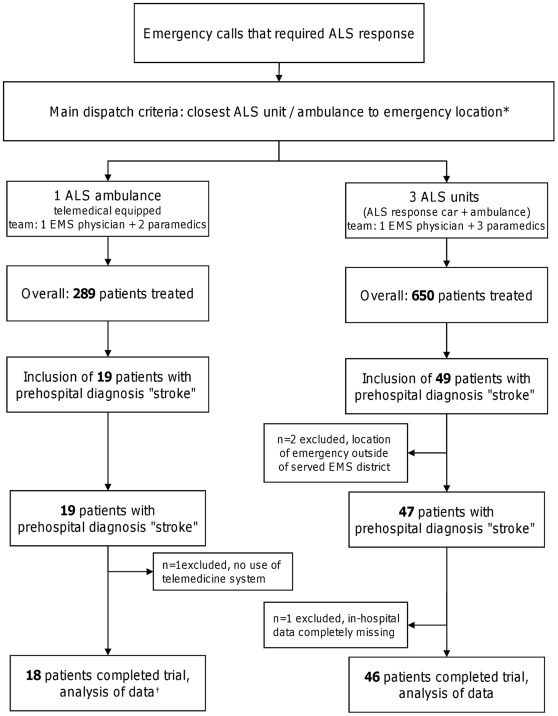
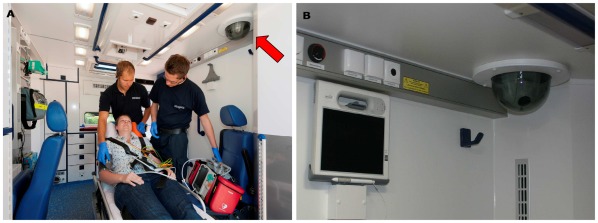
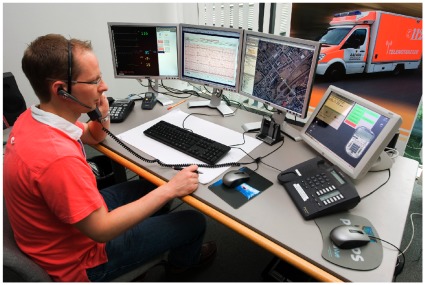
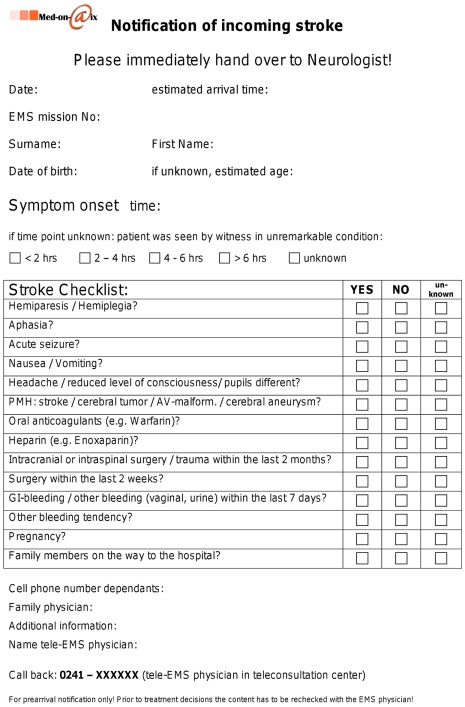
Methodology/principal findings: Teleconsultation enabling audio communication, real-time video streaming, vital data and still picture transmission was conducted between an ambulance and a teleconsultation center. Pre-notification of the hospital was carried out with a 14-item stroke history checklist via e-mail-to-fax. Beside technical assessments possible influences on prehospital and initial in-hospital time intervals, prehospital diagnostic accuracy and the transfer of stroke specific data were investigated by comparing telemedically assisted prehospital care (telemedicine group) with local regular EMS care (control group). All prehospital stroke patients over a 5-month period were included during weekdays (7.30 a.m.-4.00 p.m.). In 3 of 18 missions partial dropouts of the system occurred; neurological co-evaluation via video transmission was conducted in 12 cases. The stroke checklist was transmitted in 14 cases (78%). Telemedicine group (n = 18) vs. control group (n = 47): Prehospital time intervals were comparable, but in both groups the door to brain imaging times were longer than recommended (median 59.5 vs. 57.5 min, p = 0.6447). The prehospital stroke diagnosis was confirmed in 61% vs. 67%, p = 0.8451. Medians of 14 (IQR 9) vs. 5 (IQR 2) stroke specific items were transferred in written form to the in-hospital setting, p<0.0001. In 3 of 10 vs. 5 of 27 patients with cerebral ischemia thrombolytics were administered, p = 0.655.
Conclusions: Teleconsultation was feasible but technical performance and reliability have to be improved. The approach led to better stroke specific information; however, a superiority over regular EMS care was not found and in-hospital time intervals were unacceptably long in both groups. The feasibility of prehospital tele-stroke consultation has future potential to improve emergency care especially when no highly trained personnel are on-scene.
Trial registration: International Standard Randomised Controlled Trial Number Register (ISRCTN) ISRCTN83270177.
Conflict of interest statement
Figures
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, et al. Heart disease and stroke statistics–2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Heuschmann PU, Wiedmann S, Wellwood I, Rudd A, Di Carlo A, et al. Three-month stroke outcome: the European Registers of Stroke (EROS) investigators. Neurology. 2010;76:159–165. - PubMed
-
- Capampangan DJ, Wellik KE, Bobrow BJ, Aguilar MI, Ingall TJ, et al. Telemedicine versus telephone for remote emergency stroke consultations: a critically appraised topic. Neurologist. 2009;15:163–166. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
