

Correlation of mycobacterium tuberculosis specific and non-specific quantitative Th1 T-cell responses with bacillary load in a high burden setting
- PMID: 22629395
- PMCID: PMC3358317
- DOI: 10.1371/journal.pone.0037436
Correlation of mycobacterium tuberculosis specific and non-specific quantitative Th1 T-cell responses with bacillary load in a high burden setting
Abstract
Background: Measures of bacillary load in patients with tuberculosis (TB) may be useful for predicting and monitoring response to treatment. The relationship between quantitative T-cell responses and mycobacterial load remains unclear. We hypothesised that, in a HIV-prevalent high burden setting, the magnitude of mycobacterial antigen-specific and non-specific T-cell IFN-γ responses would correlate with (a) bacterial load and (b) culture conversion in patients undergoing treatment.
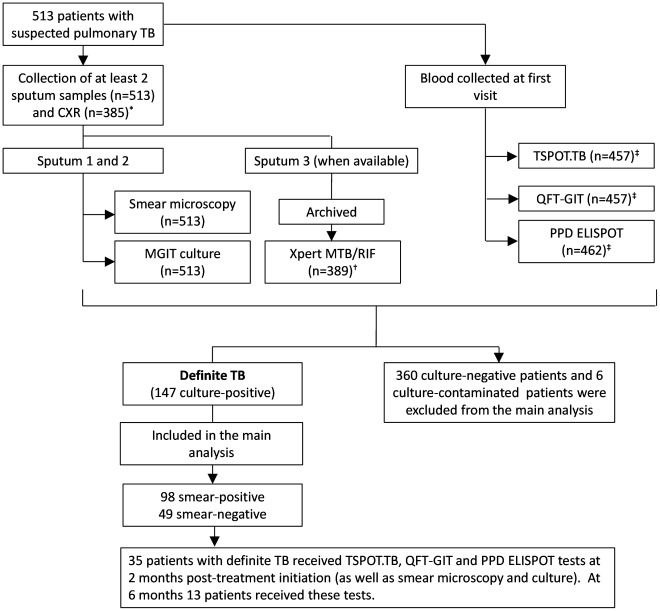
Methods: We compared baseline (n = 147), 2 (n = 35) and 6 month (n = 13) purified-protein-derivative (PPD) and RD1-specific (TSPOT.TB and QFT-GIT) blood RD1-specific (TSPOT.TB; QFT-GIT) responses with associates of sputum bacillary load in patients with culture-confirmed TB in Cape Town, South Africa.
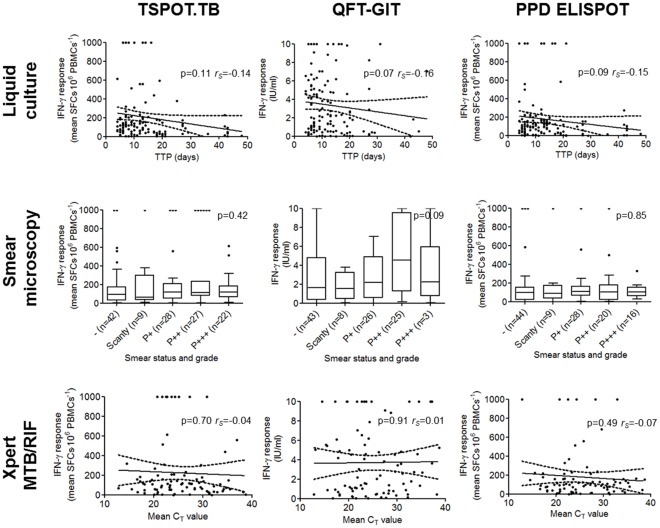
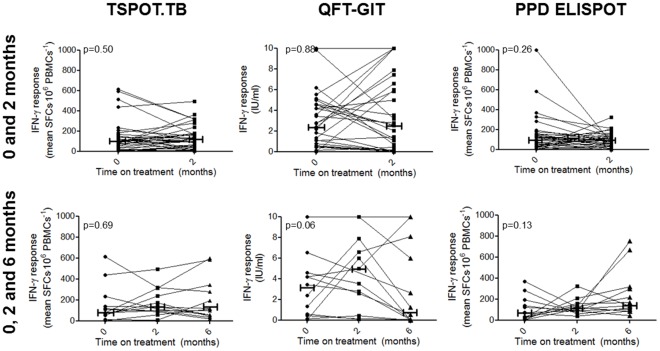
Results: IFN-γ responses were not associated with liquid culture time-to-positivity, smear-grade, Xpert MTB/RIF-generated cycle threshold values or the presence of cavities on the chest radiograph in patients with culture-confirmed TB and irrespective of HIV-status. 2-month IGRA conversion rates (positive-to-negative) were negligible [<11% for TSPOT.TB (3/28) and QFT-GIT (1/29)] and lower compared to culture [60% (21/35); p<0.01].
Conclusions: In a high burden HIV-prevalent setting T-cell IFN-γ responses to M. tuberculosis-specific and non-specific antigens do not correlate with bacillary load, including Xpert MTB/RIF-generated C(T) values, and are therefore poorly suited for monitoring treatment and prognostication.
Conflict of interest statement
Figures
References
-
- Lalvani A. Counting antigen-specific T cells: a new approach for monitoring response to tuberculosis treatment? Clinical Infectious Diseases. 2004;38:757. - PubMed
-
- WHO . Publication number WHO/HTM/TB/2011. World Health Organization, Geneva, Switzerland; 2011. Commercial Serodiagnostic Tests for Diagnosis of Tuberculosis. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
