

Early versus late parenteral nutrition in ICU patients: cost analysis of the EPaNIC trial
- PMID: 22632574
- PMCID: PMC3580642
- DOI: 10.1186/cc11361
Early versus late parenteral nutrition in ICU patients: cost analysis of the EPaNIC trial
Abstract
Introduction: The EPaNIC randomized controlled multicentre trial showed that postponing initiation of parenteral nutrition (PN) in ICU-patients to beyond the first week (Late-PN) enhanced recovery, as compared with Early-PN. This was mediated by fewer infections, accelerated recovery from organ failure and reduced duration of hospitalization. Now, the trial's preplanned cost analysis (N = 4640) from the Belgian healthcare payers' perspective is reported.
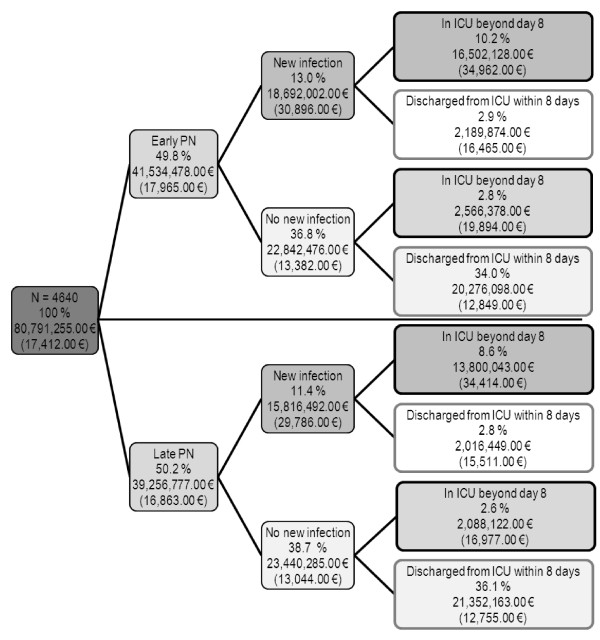
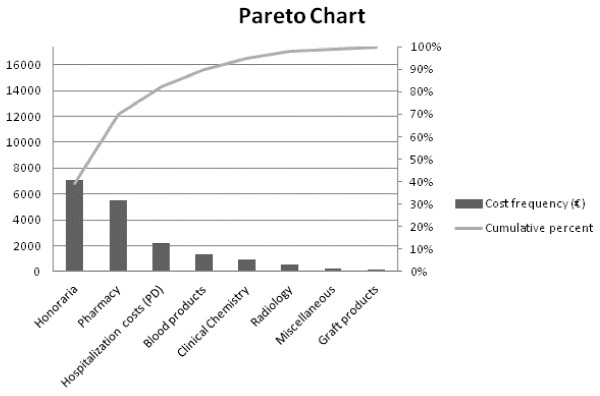
Methods: Cost data were retrieved from individual patient invoices. Undiscounted total healthcare costs were calculated for the index hospital stay. A cost tree based on acquisition of new infections and on prolonged length-of-stay was constructed. Contribution of 8 cost categories to total hospitalization costs was analyzed. The origin of drug costs was clarified in detail through the Anatomical Therapeutic Chemical (ATC) classification system. The potential impact of Early-PN on total hospitalization costs in other healthcare systems was explored in a sensitivity analysis.
Results: ICU-patients developing new infection (24.4%) were responsible for 42.7% of total costs, while ICU-patients staying beyond one week (24.3%) accounted for 43.3% of total costs. Pharmacy-related costs represented 30% of total hospitalization costs and were increased by Early-PN (+608.00 EUR/patient, p = 0.01). Notably, costs for ATC-J (anti-infective agents) (+227.00 EUR/patient, p = 0.02) and ATC-B (comprising PN) (+220.00 EUR/patient, p = 0.006) drugs were increased by Early-PN. Sensitivity analysis revealed a mean total cost increase of 1,210.00 EUR/patient (p = 0.02) by Early-PN, when incorporating the full PN costs.
Conclusions: The increased costs by Early-PN were mainly pharmacy-related and explained by higher expenditures for PN and anti-infective agents. The use of Early-PN in critically ill patients can thus not be recommended for both clinical (no benefit) and cost-related reasons.
Trial registration: ClinicalTrials.gov NCT00512122.
Figures
References
-
- Dhaliwal R, Jurewitsch B, Harrietha D, Heyland DK. Combination enteral and parenteral nutrition in critically ill patients: harmful or beneficial? A systematic review of the evidence. Intensive Care Med. 2004;30:1666–1671. - PubMed
-
- Casaer MP, Mesotten D, Hermans G, Wouters PJ, Schetz M, Meyfroidt G, Van Cromphaut S, Ingels C, Meersseman P, Muller J, Vlasselaers D, Debaveye Y, Desmet L, Dubois J, Van Assche A, Vanderheyden S, Wilmer A, Van den Berghe G. Early versus late parenteral nutrition in critically ill adults. N Engl J Med. 2011;365:506–517. doi: 10.1056/NEJMoa1102662. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
