

Recombinant tissue plasminogen activator for acute ischaemic stroke: an updated systematic review and meta-analysis
- PMID: 22632907
- PMCID: PMC3386494
- DOI: 10.1016/S0140-6736(12)60738-7
Recombinant tissue plasminogen activator for acute ischaemic stroke: an updated systematic review and meta-analysis
Abstract
Background: Recombinant tissue plasminogen activator (rt-PA, alteplase) improved functional outcome in patients treated soon after acute ischaemic stroke in randomised trials, but licensing is restrictive and use varies widely. The IST-3 trial adds substantial new data. We therefore assessed all the evidence from randomised trials for rt-PA in acute ischaemic stroke in an updated systematic review and meta-analysis.
Methods: We searched for randomised trials of intravenous rt-PA versus control given within 6 h of onset of acute ischaemic stroke up to March 30, 2012. We estimated summary odds ratios (ORs) and 95% CI in the primary analysis for prespecified outcomes within 7 days and at the final follow-up of all patients treated up to 6 h after stroke.
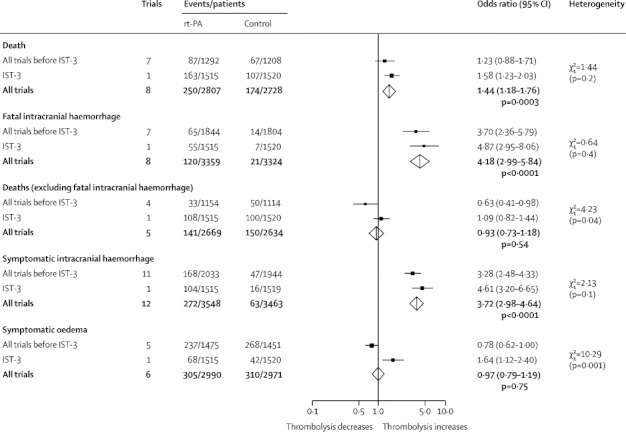
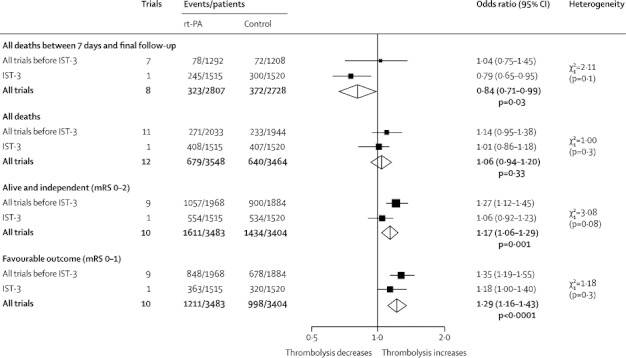
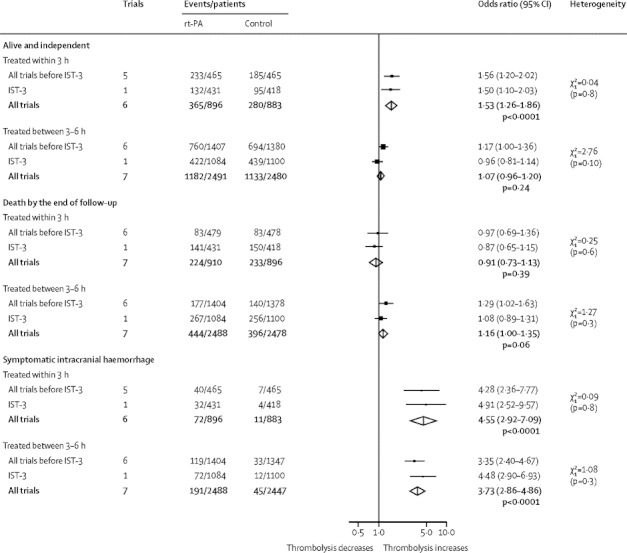
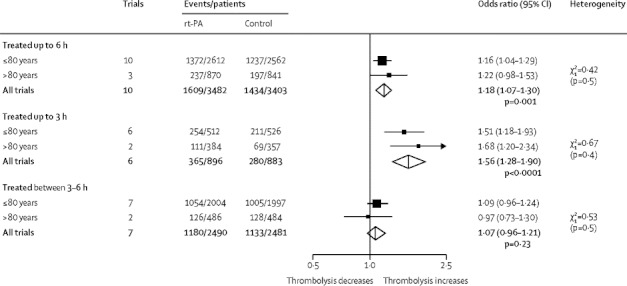
Findings: In up to 12 trials (7012 patients), rt-PA given within 6 h of stroke significantly increased the odds of being alive and independent (modified Rankin Scale, mRS 0-2) at final follow-up (1611/3483 [46·3%] vs 1434/3404 [42·1%], OR 1·17, 95% CI 1·06-1·29; p=0·001), absolute increase of 42 (19-66) per 1000 people treated, and favourable outcome (mRS 0-1) absolute increase of 55 (95% CI 33-77) per 1000. The benefit of rt-PA was greatest in patients treated within 3 h (mRS 0-2, 365/896 [40·7%] vs 280/883 [31·7%], 1·53, 1·26-1·86, p<0·0001), absolute benefit of 90 (46-135) per 1000 people treated, and mRS 0-1 (283/896 [31·6%] vs 202/883 [22·9%], 1·61, 1·30-1·90; p<0·0001), absolute benefit 87 (46-128) per 1000 treated. Numbers of deaths within 7 days were increased (250/2807 [8·9%] vs 174/2728 [6·4%], 1·44, 1·18-1·76; p=0·0003), but by final follow-up the excess was no longer significant (679/3548 [19·1%] vs 640/3464 [18·5%], 1·06, 0·94-1·20; p=0·33). Symptomatic intracranial haemorrhage (272/3548 [7·7%] vs 63/3463 [1·8%], 3·72, 2·98-4·64; p<0·0001) accounted for most of the early excess deaths. Patients older than 80 years achieved similar benefit to those aged 80 years or younger, particularly when treated early.
Interpretation: The evidence indicates that intravenous rt-PA increased the proportion of patients who were alive with favourable outcome and alive and independent at final follow-up. The data strengthen previous evidence to treat patients as early as possible after acute ischaemic stroke, although some patients might benefit up to 6 h after stroke.
Funding: UK Medical Research Council, Stroke Association, University of Edinburgh, National Health Service Health Technology Assessment Programme, Swedish Heart-Lung Fund, AFA Insurances Stockholm (Arbetsmarknadens Partners Forsakringsbolag), Karolinska Institute, Marianne and Marcus Wallenberg Foundation, Research Council of Norway, Oslo University Hospital.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
rt-PA for ischaemic stroke: what will the next question be?Lancet. 2012 Jun 23;379(9834):2320-1. doi: 10.1016/S0140-6736(12)60822-8. Epub 2012 May 23. Lancet. 2012. PMID: 22632906 No abstract available.
References
-
- The National Institute of Neurological Disorders and Stroke (NINDS) rt-PA Stroke Study Group Tissue plasminogen activator for acute ischaemic stroke. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Hacke W, Kaste M, Fieschi C. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS) JAMA. 1995;274:1017–1025. - PubMed
-
- Hacke W, Kaste M, Fieschi C. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II) Lancet. 1998;352:1245–1251. - PubMed
-
- Wardlaw JM, Sandercock PAG, Berge E. Thrombolytic therapy with recombinant tissue plasminogen activator for acute ischemic stroke. Where do we go from here? A cumulative meta-analysis. Stroke. 2003;34:1437–1442. - PubMed
-
- Wardlaw JM, del Zoppo G, Yamaguchi T, Berge E. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev. 2003 CD000213. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
