

Evaluating age in the field triage of injured persons
- PMID: 22633339
- PMCID: PMC3428427
- DOI: 10.1016/j.annemergmed.2012.04.006
Evaluating age in the field triage of injured persons
Abstract
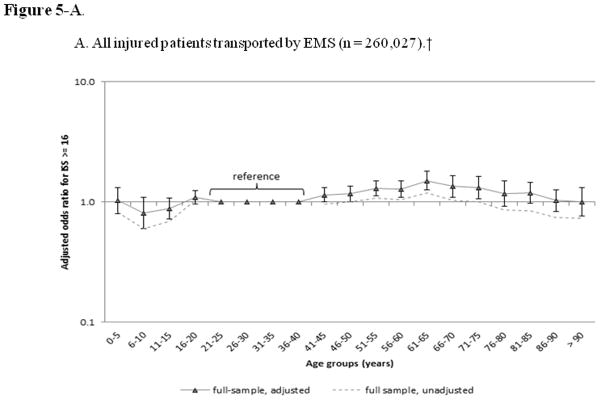
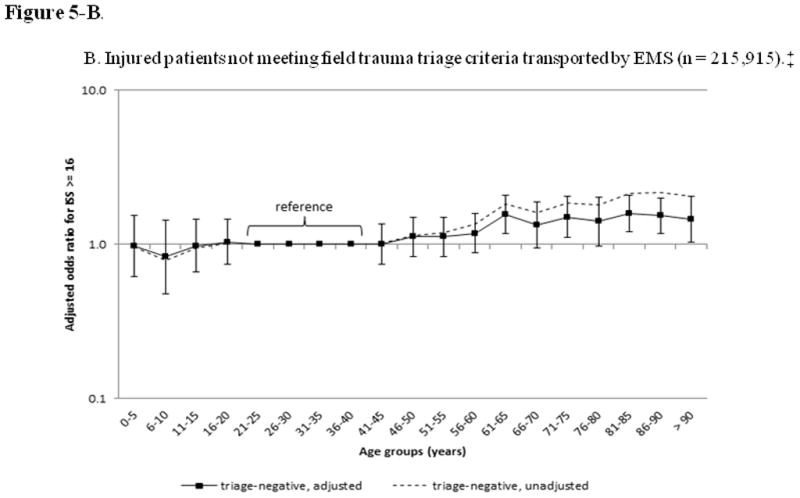
Study objective: We evaluate trauma undertriage by age group, the association between age and serious injury after accounting for other field triage criteria and confounders, and the potential effect of a mandatory age triage criterion for field triage.
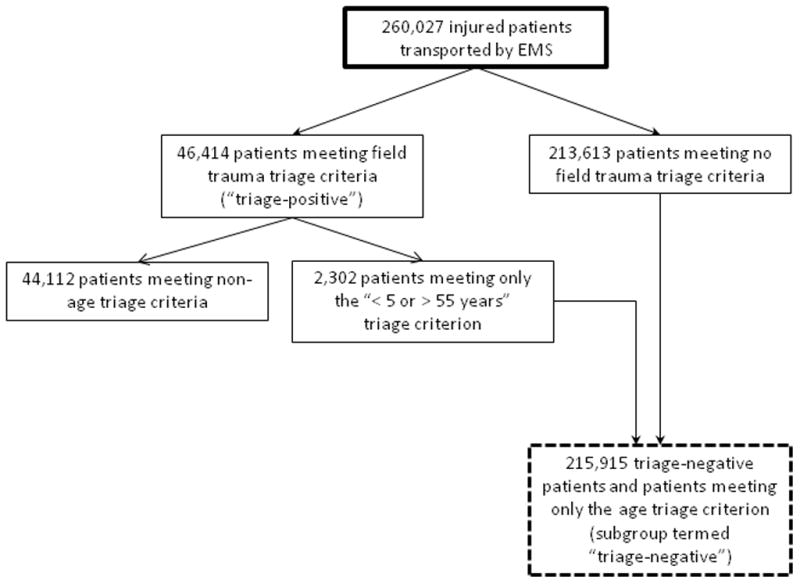
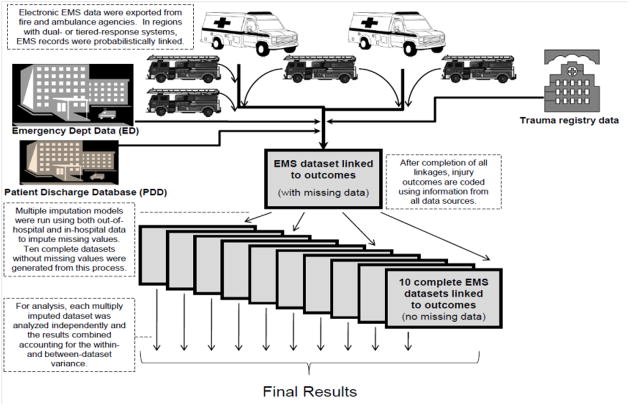
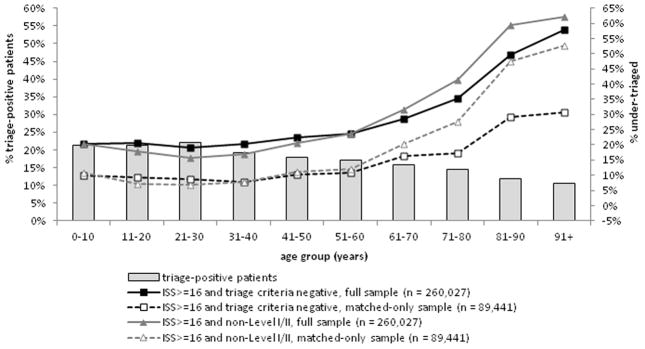
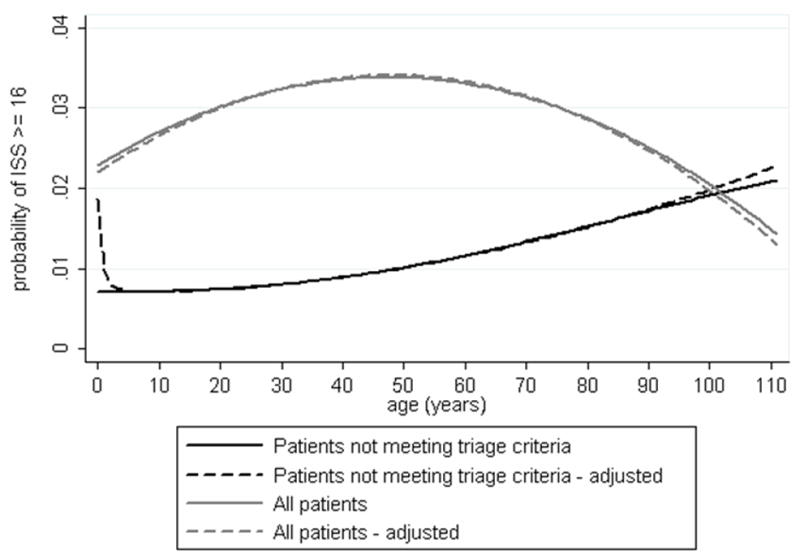
Methods: This was a retrospective cohort study of injured children and adults transported by 48 emergency medical services (EMS) agencies to 105 hospitals in 6 regions of the western United States from 2006 through 2008. We used probabilistic linkage to match EMS records to hospital records, including trauma registries, state discharge databases, and emergency department databases. The primary outcome measure was serious injury, as measured by an Injury Severity Score greater than or equal to 16. We assessed undertriage (Injury Severity Score ≥16 and triage-negative or transport to a nontrauma center) by age decile and used multivariable logistic regression models to estimate the association (linear and nonlinear) between age and Injury Severity Score greater than or equal to 16, adjusted for important confounders. We also evaluated the potential influence of age on triage efficiency and trauma center volume.
Results: Injured patients (260,027) were evaluated and transported by EMS during the 3-year study period. Undertriage increased for patients older than 60 years, reaching approximately 60% for those older than 90 years. There was a strong nonlinear association between age and Injury Severity Score greater than or equal to 16. For patients not meeting other triage criteria, the probability of serious injury was most notable after 60 years. A mandatory age triage criterion would have decreased undertriage at the expense of overtriage, with 1 patient with Injury Severity Score greater than or equal to 16 identified for every 60 to 65 additional patients transported to major trauma centers.
Conclusion: Trauma undertriage increases in patients older than 60 years. Although the probability of serious injury increases among triage-negative patients with increasing age, the use of a mandatory age triage criterion appears inefficient for improving field triage.
Copyright © 2012. Published by Mosby, Inc.
Figures
References
-
- MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. NEJM. 2006;354:366–378. - PubMed
-
- Centers for Disease Control and Prevention. Guidelines for Field Triage of Injured Patients: Recommendations of the National Expert Panel on Field Triage. MMWR. 2009;58:1–35. - PubMed
-
- Resources for the Optimal Care of the Injured Patient. Chicago, IL: American College of Surgeons; 2006.
-
- Mackersie RC. History of trauma field triage development and the American College of Surgeons criteria. Prehospital Emergency Care. 2006;10:287–294. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
