

Evaluation of failure to rescue as a quality metric in pediatric heart surgery: an analysis of the STS Congenital Heart Surgery Database
- PMID: 22633496
- PMCID: PMC3828205
- DOI: 10.1016/j.athoracsur.2012.03.065
Evaluation of failure to rescue as a quality metric in pediatric heart surgery: an analysis of the STS Congenital Heart Surgery Database
Abstract
Background: Failure to rescue (FTR; the probability of death after a complication) has been adopted as a quality metric in adult cardiac surgery, in which it has been shown that high-performing centers with low mortality rates do not have fewer complications, but rather lower mortality in those who experience a complication (lower FTR). It is unknown whether this holds true in pediatric heart surgery. We characterized the relationship between complications, FTR, and mortality in this population.
Methods: Children (0 to 18 years) undergoing heart surgery at centers participating in the Society of Thoracic Surgeons Congenital Heart Surgery Database (2006 to 2009) were included. Outcomes were examined in multivariable analysis adjusting for patient characteristics, surgical risk category, and within-center clustering.
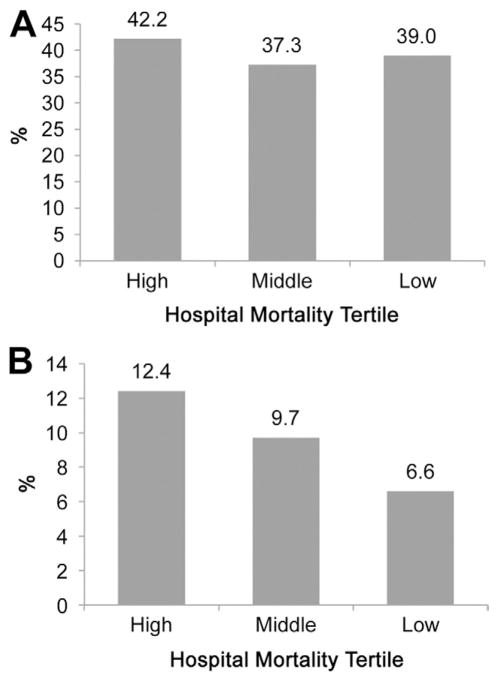
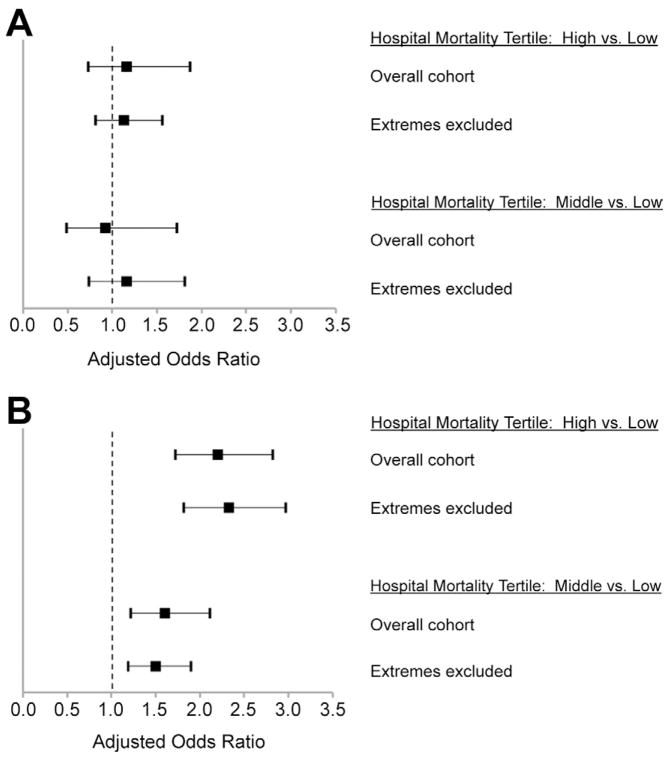
Results: This study included 40,930 patients from 72 centers. Overall in-hospital mortality was 3.7%, 39.3% had a postoperative complication, and the FTR rate (number of deaths in those with a complication) was 9.1%. When hospitals were characterized by in-hospital mortality rate, there was no difference across hospital mortality tertiles in the complication rate in adjusted analysis; however, hospitals in the lowest mortality tertile had significantly lower FTR rates (6.6% versus 12.4%; p<0.0001). Similar results were seen when evaluating high-severity complications and across surgical risk groups.
Conclusions: This analysis suggests that hospitals with low mortality rates do not have fewer complications after pediatric heart surgery, but instead have lower mortality in those who experience a complication (lower FTR). Further investigation into FTR as a quality metric in pediatric heart surgery is warranted.
Copyright © 2012 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Centers for Medicare & Medicaid Services. [Accessed November 30, 2011];Hospital–acquired conditions (present on admission indicator) Available at: http://www.cms.gov/HospitalAcqCond/
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. New Engl J Med. 2009;361:1368–75. - PubMed
-
- Silber JH, Williams SV, Krakauer H, Schwartz JS. Hospital and patient characteristics associated with death after surgery: a study of adverse occurrence and failure to rescue. Med Care. 1992;30:615–29. - PubMed
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Complications, failure to rescue, and mortality with major inpatient surgery in Medicare patients. Ann Surg. 2009;250:1029–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
