

Role of intensive glucose control in development of renal end points in type 2 diabetes mellitus: systematic review and meta-analysis intensive glucose control in type 2 diabetes
- PMID: 22636820
- PMCID: PMC3688081
- DOI: 10.1001/archinternmed.2011.2230
Role of intensive glucose control in development of renal end points in type 2 diabetes mellitus: systematic review and meta-analysis intensive glucose control in type 2 diabetes
Erratum in
- Arch Intern Med. 2012 Jul 23;172(14):1095
Abstract
Background: Aggressive glycemic control has been hypothesized to prevent renal disease in patients with type 2 diabetes mellitus. A systematic review was conducted to summarize the benefits of intensive vs conventional glucose control on kidney-related outcomes for adults with type 2 diabetes.
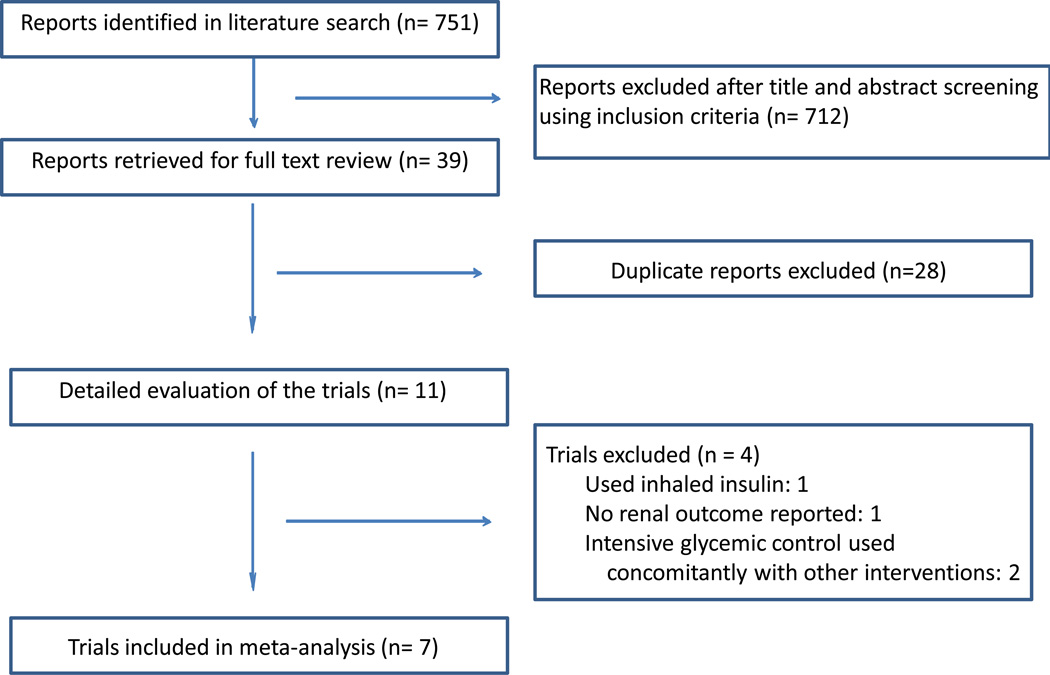
Methods: Three databases were systematically searched (January 1, 1950, to December 31, 2010) with no language restrictions to identify randomized trials that compared surrogate renal end points (microalbuminuria and macroalbuminuria) and clinical renal end points (doubling of the serum creatinine level, end-stage renal disease [ESRD], and death from renal disease) in patients with type 2 diabetes receiving intensive glucose control vs those receiving conventional glucose control.
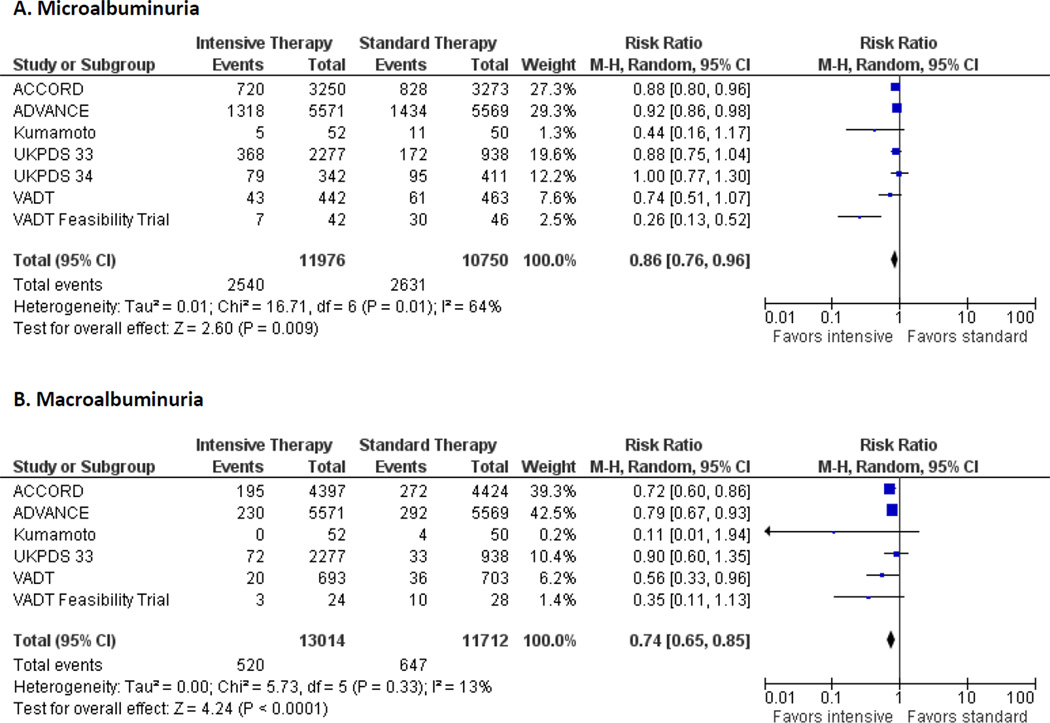
Results: We evaluated 7 trials involving 28 065 adults who were monitored for 2 to 15 years. Compared with conventional control, intensive glucose control reduced the risk for microalbuminuria (risk ratio, 0.86 [95% CI, 0.76-0.96]) and macroalbuminuria (0.74 [0.65-0.85]), but not doubling of the serum creatinine level (1.06 [0.92-1.22]), ESRD (0.69 [0.46-1.05]), or death from renal disease (0.99 [0.55-1.79]). Meta-regression revealed that larger differences in hemoglobin A1c between intensive and conventional therapy at the study level were associated with greater benefit for both microalbuminuria and macroalbuminuria. The pooled cumulative incidence of doubling of the serum creatinine level, ESRD, and death from renal disease was low (<4%, <1.5%, and <0.5%, respectively) compared with the surrogate renal end points of microalbuminuria (23%) and macroalbuminuria (5%).
Conclusions: Intensive glucose control reduces the risk for microalbuminuria and macroalbuminuria, but evidence is lacking that intensive glycemic control reduces the risk for significant clinical renal outcomes, such as doubling of the serum creatinine level, ESRD, or death from renal disease during the years of follow-up of the trials.
Figures

Comment in
-
Understanding the long-term benefits and dangers of intensive therapy of diabetes.Arch Intern Med. 2012 May 28;172(10):769-70. doi: 10.1001/archinternmed.2012.438. Arch Intern Med. 2012. PMID: 22636821 No abstract available.
-
Prioritizing treatments in type 2 diabetes mellitus.Arch Intern Med. 2012 May 28;172(10):770-2. doi: 10.1001/archinternmed.2012.1775. Arch Intern Med. 2012. PMID: 22636822 No abstract available.
-
Intensive glucose control in patients with type 2 diabetes is associated with a reduction in albuminuria and may be associated with reduced end-stage renal disease.Evid Based Med. 2013 Jun;18(3):105-6. doi: 10.1136/eb-2012-100904. Epub 2012 Aug 29. Evid Based Med. 2013. PMID: 22933548 No abstract available.
-
ACP Journal Club. Review: intensive glucose control reduces surrogate, but not clinical, renal outcomes in type 2 diabetes.Ann Intern Med. 2012 Nov 20;157(10):JC5-6. doi: 10.7326/0003-4819-157-10-201211200-02006. Ann Intern Med. 2012. PMID: 23165682 No abstract available.
References
-
- Kawazu S, Tomono S, Shimizu M, et al. The relationship between early diabetic nephropathy and control of plasma glucose in non-insulin-dependent diabetes mellitus. The effect of glycemic control on the development and progression of diabetic nephropathy in an 8-year follow-up study. J Diabetes Complications. 1994;8(1):13–17. [8167381] - PubMed
-
- The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329(14):977–986. [8366922] - PubMed
-
- Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28(2):103–117. [7587918] - PubMed
-
- Levin SR, Coburn JW, Abraira C, et al. Effect of intensive glycemic control on microalbuminuria in type 2 diabetes. Veterans Affairs Cooperative Study on Glycemic Control and Complications in Type 2 Diabetes Feasibility Trial Investigators. Diabetes Care. 2000;23(10):1478–1485. [11023140] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
