

The locking attachment plate for proximal fixation of periprosthetic femur fractures--a biomechanical comparison of two techniques
- PMID: 22638607
- PMCID: PMC3427437
- DOI: 10.1007/s00264-012-1574-x
The locking attachment plate for proximal fixation of periprosthetic femur fractures--a biomechanical comparison of two techniques
Abstract
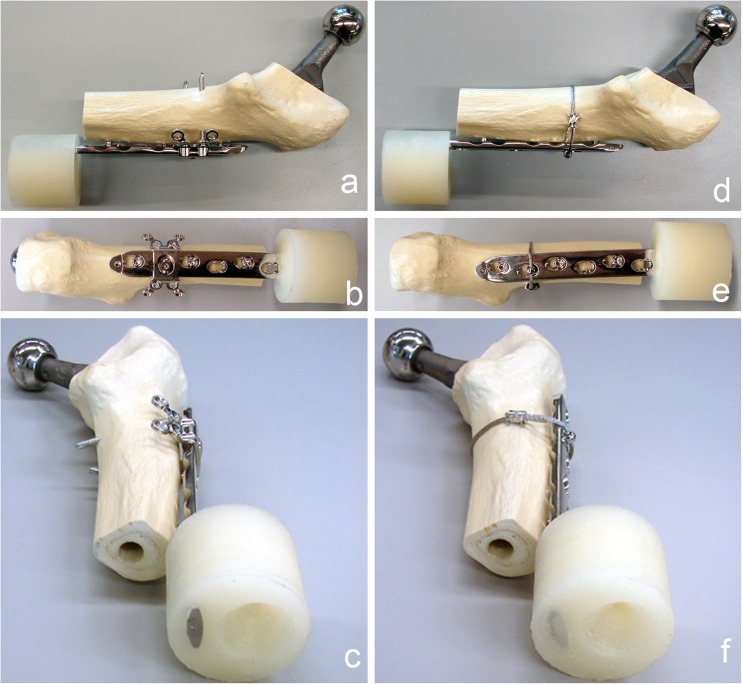
Purpose: Mechanical properties of a locking attachment plate construct (LAP-LCP), allowing bicortical screw placement laterally to the prosthesis stem, are compared to a cerclage-LCP construct.
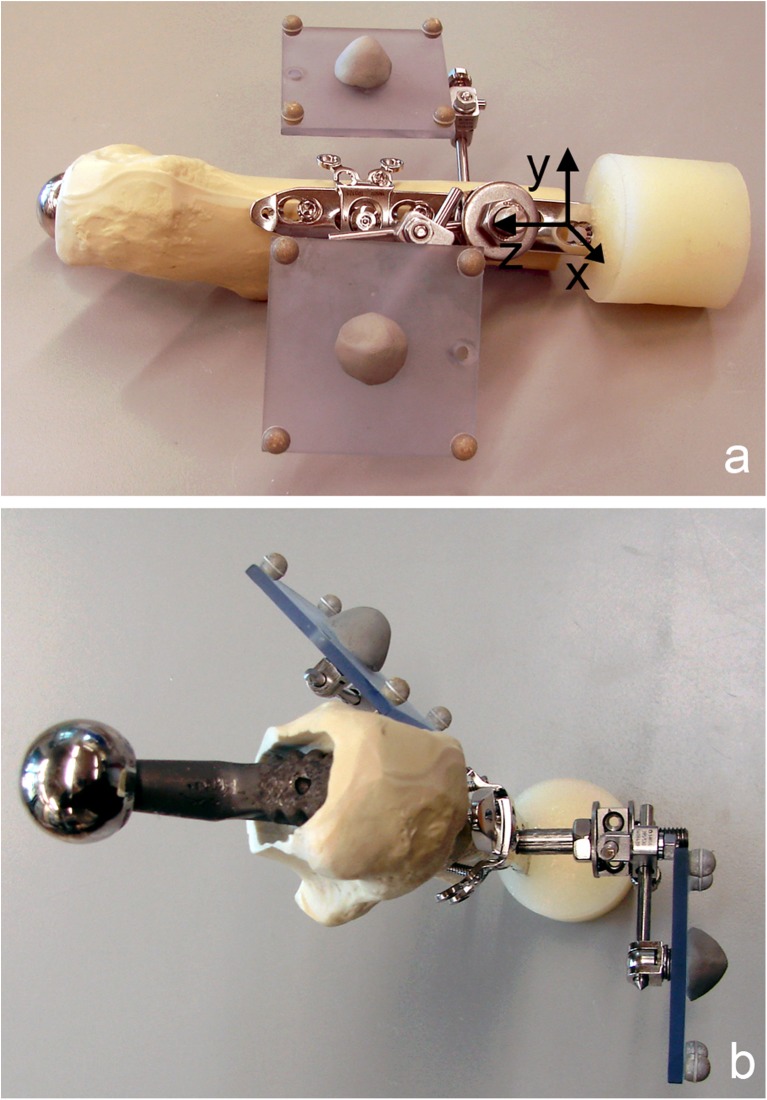
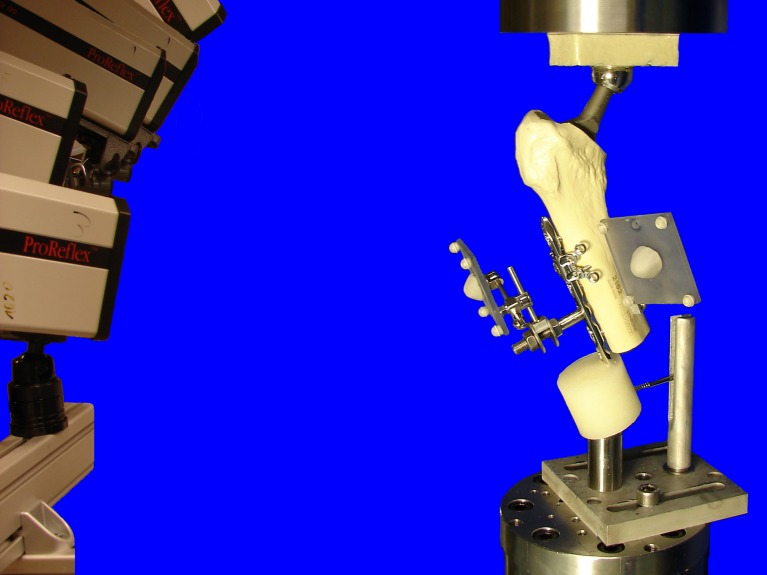
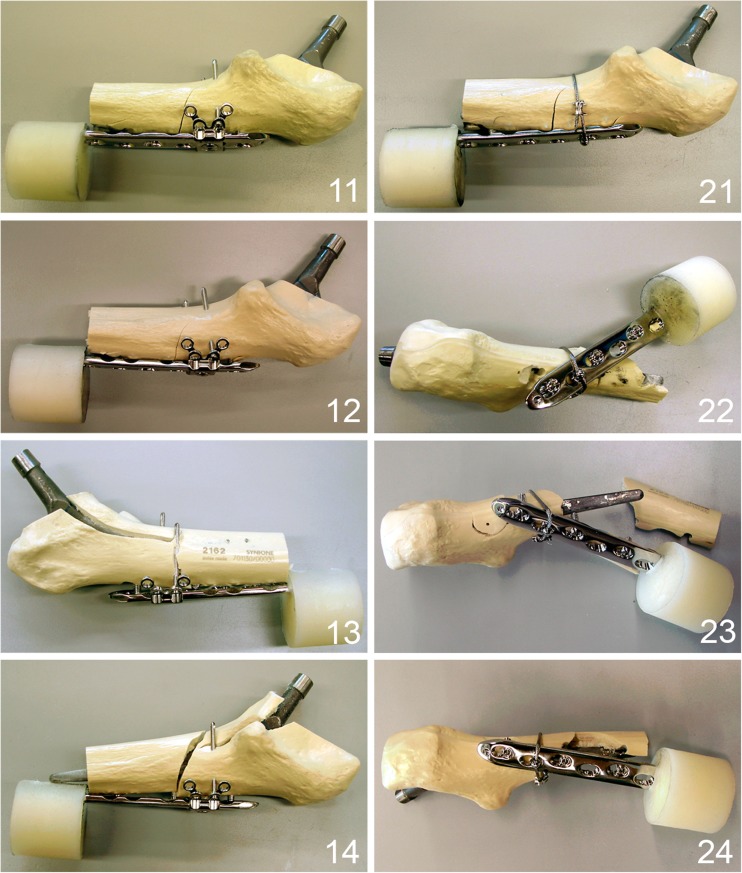
Methods: Eight right synthetic femora with implanted uncemented hip endoprosthesis were cut distally and fixed with LCP, monocortical locking screws and either LAP (n = 4) or cerclage (n = 4). Cyclic testing was performed with monotonically increasing sinusoidal load until failure. Relative movements at the plate-femur interface were registered by motion tracking. Statistical differences were detected by unpaired t-test and general linear model repeated measures.
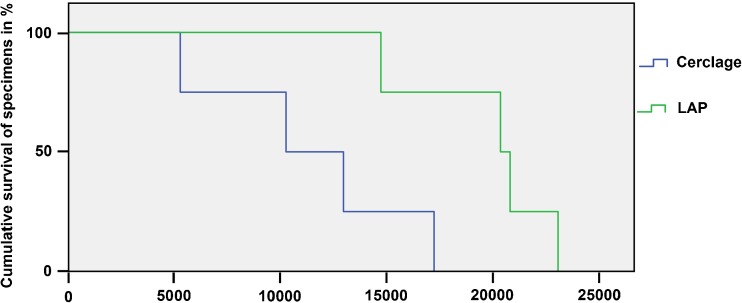
Results: Stiffness of the LAP-LCP was significantly higher at the beginning (875.4 N/mm ± 29.8) and after 5000 cycles (1213.0 N/mm ± 101.1) compared to the cerclage-LCP (644.96 N/mm ± 50.1 and 851.9 N/mm ± 81.9), with p = 0.013. Relative movements for AP-bending (B) and axial translation (T) of the LAP-LCP at the beginning (0.07° ± 0.02, 0.20 mm ± 0.08), after 500 cycles (0.16° ± 0.10, 0.26 mm ± 0.07) and after 5000 cycles (0.26° ± 0.11, 0.31 mm ± 0.07) differed significantly from the cerclage-LCP (beg.: 0.26° ± 0.04, 0.28 mm ± 0.05; 500 cyc: 0.47° ± 0.03, 0.53 mm ± 0.07; 5000 cyc.: 0.63° ± 0.18, 0.79 mm ± 0.13), with B: p = 0.02, T: p = 0.04. Relative movements for medial bending were not significantly different between the two constructs. Cycles to failure (criterion 1 mm axial translation) differed significantly between LAP-LCP (19,519 ± 1,758) and cerclage-LCP (11,265 ± 2,472), with p = 0.035.
Conclusions: Biomechanically, the LAP-LCP construct improves proximal fixation of periprosthetic fractures compared to the cerclage-LCP construct.
Figures
References
-
- Duncan CP, Masri BA. Fractures of the femur after hip replacement. Instr Course Lect. 1995;44:293–304. - PubMed
-
- Pike J, Davidson D, Garbuz D, Duncan CP, O’Brien PJ, Masri BA. Principles of treatment for periprosthetic femoral shaft fractures around well-fixed total hip arthroplasty. J Am Acad Orthop Surg. 2009;17:677–688. - PubMed
-
- Virolainen P, Mokka J, Seppanen M, Makela K. Up to 10 years follow up of the use of 71 cortical allografts (strut-grafts) for the treatment of periprosthetic fractures. Scand J Surg. 2010;99:240–243. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
