

Cherubism: best clinical practice
- PMID: 22640403
- PMCID: PMC3359956
- DOI: 10.1186/1750-1172-7-S1-S6
Cherubism: best clinical practice
Abstract
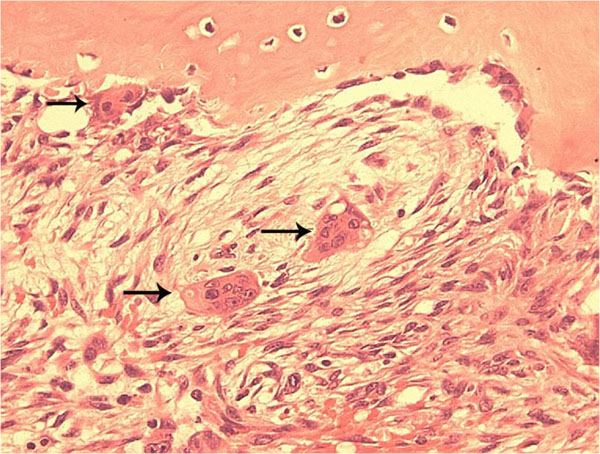
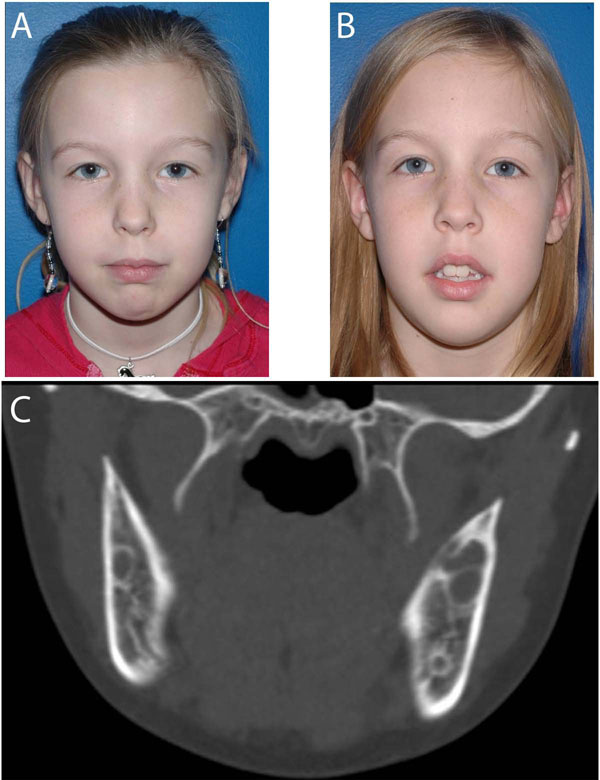
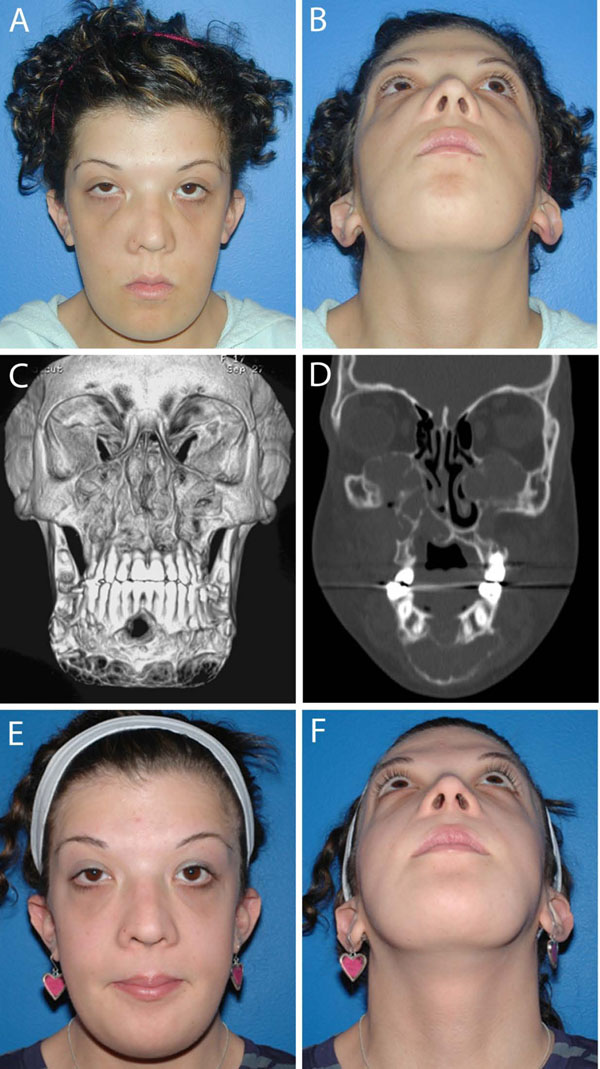
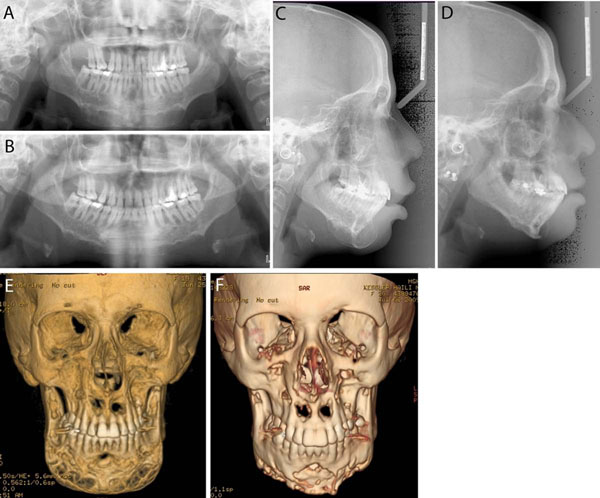
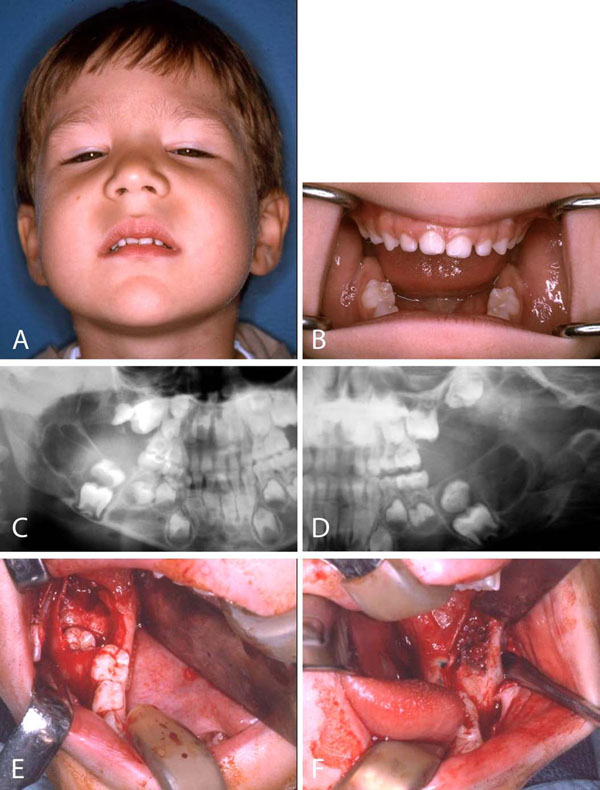
Cherubism is a skeletal dysplasia characterized by bilateral and symmetric fibro-osseous lesions limited to the mandible and maxilla. In most patients, cherubism is due to dominant mutations in the SH3BP2 gene on chromosome 4p16.3. Affected children appear normal at birth. Swelling of the jaws usually appears between 2 and 7 years of age, after which, lesions proliferate and increase in size until puberty. The lesions subsequently begin to regress, fill with bone and remodel until age 30, when they are frequently not detectable.Fibro-osseous lesions, including those in cherubism have been classified as quiescent, non-aggressive and aggressive on the basis of clinical behavior and radiographic findings. Quiescent cherubic lesions are usually seen in older patients and do not demonstrate progressive growth. Non-aggressive lesions are most frequently present in teenagers. Lesions in the aggressive form of cherubism occur in young children and are large, rapidly growing and may cause tooth displacement, root resorption, thinning and perforation of cortical bone.Because cherubism is usually self-limiting, operative treatment may not be necessary. Longitudinal observation and follow-up is the initial management in most cases. Surgical intervention with curettage, contouring or resection may be indicated for functional or aesthetic reasons. Surgical procedures are usually performed when the disease becomes quiescent. Aggressive lesions that cause severe functional problems such as airway obstruction justify early surgical intervention.
Figures
References
-
- Jones WA. Familial multilocular cystic disease of the jaws. American Journal of Cancer. 1933;17:946–950.
-
- Jones WA. Further observations regarding familal multilocular cystic disease of the jaws. British Journal of Radiology. 1938;11:227–241. doi: 10.1259/0007-1285-11-124-227. - DOI
-
- Jones WA, Gerrie J, Pritchard J. Cherubism--familial fibrous dysplasia of the jaws. Journal of Bone and Joint Surgery. British Volume. 1950;32-B(3):334–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
