

Variation in cancer surgical outcomes associated with physician and nurse staffing: a retrospective observational study using the Japanese Diagnosis Procedure Combination Database
- PMID: 22640411
- PMCID: PMC3405470
- DOI: 10.1186/1472-6963-12-129
Variation in cancer surgical outcomes associated with physician and nurse staffing: a retrospective observational study using the Japanese Diagnosis Procedure Combination Database
Abstract
Background: Little is known about the effects of professional staffing on cancer surgical outcomes. The present study aimed to investigate the association between cancer surgical outcomes and physician/nurse staffing in relation to hospital volume.
Methods: We analyzed 131,394 patients undergoing lung lobectomy, esophagectomy, gastrectomy, colorectal surgery, hepatectomy or pancreatectomy for cancer between July and December, 2007-2008, using the Japanese Diagnosis Procedure Combination database linked to the Survey of Medical Institutions data. Physician-to-bed ratio (PBR) and nurse-to-bed ratio (NBR) were determined for each hospital. Hospital volume was categorized into low, medium and high for each of six cancer surgeries. Failure to rescue (FTR) was defined as a proportion of inhospital deaths among those with postoperative complications. Multi-level logistic regression analysis was performed to examine the association between physician/nurse staffing and FTR, adjusting for patient characteristics and hospital volume.
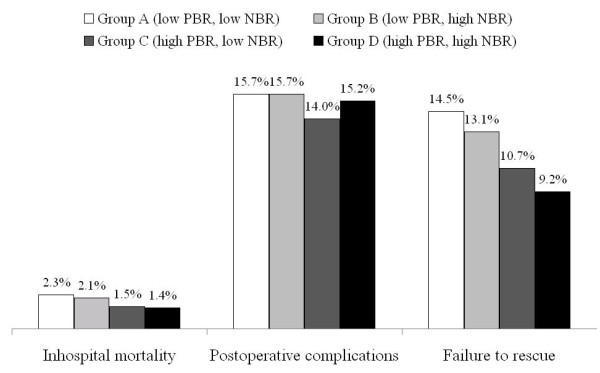
Results: Overall inhospital mortality was 1.8%, postoperative complication rate was 15.2%, and FTR rate was 11.9%. After adjustment for hospital volume, FTR rate in the group with high PBR (≥19.7 physicians per 100 beds) and high NBR (≥77.0 nurses per 100 beds) was significantly lower than that in the group with low PBR (<19.7) and low NBR (<77.0) (9.2% vs. 14.5%; odds ratio, 0.76; 95% confidence interval, 0.68-0.86; p < 0.001).
Conclusions: Well-staffed hospitals confer a benefit for cancer surgical patients regarding reduced FTR, irrespective of hospital volume. These results suggest that consolidation of surgical centers linked with migration of medical professionals may improve the quality of cancer surgical management.
Figures
Similar articles
-
Procedure-Specific Volume and Nurse-to-Patient Ratio: Implications for Failure to Rescue Patients Following Liver Surgery.World J Surg. 2019 Mar;43(3):910-919. doi: 10.1007/s00268-018-4859-4. World J Surg. 2019. PMID: 30465087
-
Dose-response association between nurse staffing and patient outcomes following major cancer surgeries using a nationwide inpatient database in Japan.J Clin Nurs. 2022 Sep;31(17-18):2562-2573. doi: 10.1111/jocn.16075. Epub 2021 Oct 24. J Clin Nurs. 2022. PMID: 34693584
-
Association Between Hospital Staffing Models and Failure to Rescue.Ann Surg. 2019 Jul;270(1):91-94. doi: 10.1097/SLA.0000000000002744. Ann Surg. 2019. PMID: 29557884 Free PMC article.
-
Nurse staffing and quality of patient care.Evid Rep Technol Assess (Full Rep). 2007 Mar;(151):1-115. Evid Rep Technol Assess (Full Rep). 2007. PMID: 17764206 Free PMC article. Review.
-
Evidence of the Association between Nurse Staffing Levels and Patient and Nurses' Outcomes in Acute Care Hospitals across Japan: A Scoping Review.Healthcare (Basel). 2022 Jun 6;10(6):1052. doi: 10.3390/healthcare10061052. Healthcare (Basel). 2022. PMID: 35742103 Free PMC article.
Cited by
-
Evaluation of the Effectiveness and Use of Anti-Methicillin-Resistant Staphylococcus aureus Agents for Aspiration Pneumonia in Older Patients Using a Nationwide Japanese Administrative Database.Microorganisms. 2023 Jul 27;11(8):1905. doi: 10.3390/microorganisms11081905. Microorganisms. 2023. PMID: 37630465 Free PMC article.
-
Continuous regional arterial infusion for acute pancreatitis: a propensity score analysis using a nationwide administrative database.Crit Care. 2013 Oct 2;17(5):R214. doi: 10.1186/cc13029. Crit Care. 2013. PMID: 24088324 Free PMC article.
-
The relationship between high-dose corticosteroid treatment and mortality in acute respiratory distress syndrome: a retrospective and observational study using a nationwide administrative database in Japan.BMC Pulm Med. 2018 Feb 7;18(1):28. doi: 10.1186/s12890-018-0597-5. BMC Pulm Med. 2018. PMID: 29415701 Free PMC article.
-
In-Hospital Mortality for Hepatic Portal Venous Gas: Analysis of 1590 Patients Using a Japanese National Inpatient Database.World J Surg. 2018 Mar;42(3):816-822. doi: 10.1007/s00268-017-4189-y. World J Surg. 2018. PMID: 28879575
-
Components of Hospital Perioperative Infrastructure Can Overcome the Weekend Effect in Urgent General Surgery Procedures.Ann Surg. 2015 Oct;262(4):683-91. doi: 10.1097/SLA.0000000000001436. Ann Surg. 2015. PMID: 26366549 Free PMC article.
References
-
- Ministry of Health, Labour and Welfare, Japan. Vital statistics. , ; Accessed 30 April 2012, at http://www.mhlw.go.jp/english/database/db-hw/index.html.
-
- Ministry of Health, Labour and Welfare, Japan. Survey of Medical Institutions 2008. Accessed 30 April 2012, at http://www.mhlw.go.jp/english/database/db-hss/mi.html.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
