

A validated prediction tool for initial survivors of in-hospital cardiac arrest
- PMID: 22641228
- PMCID: PMC3517176
- DOI: 10.1001/archinternmed.2012.2050
A validated prediction tool for initial survivors of in-hospital cardiac arrest
Abstract
Background: Accurate estimation of favorable neurological survival after in-hospital cardiac arrest could provide critical information for physicians, patients, and families.
Methods: Within the Get With the Guidelines-Resuscitation registry, we identified 42,957 patients from 551 hospitals admitted between January 2000 and October 2009 who were successfully resuscitated from an in-hospital cardiac arrest. A simple prediction tool for favorable neurological survival in patients successfully resuscitated from an in-hospital cardiac arrest was developed using multivariate logistic regression, with two-thirds of the sample randomly selected as the derivation cohort and one-third as the validation cohort. Favorable neurological status was defined as the absence of severe neurological deficits (cerebral performance category score of ≤2).
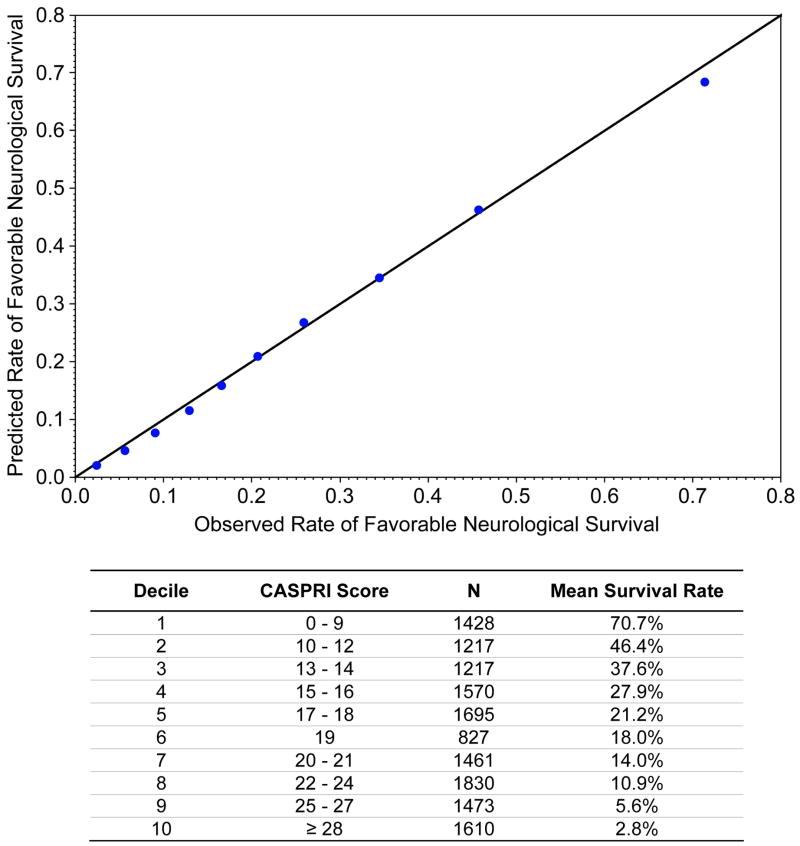
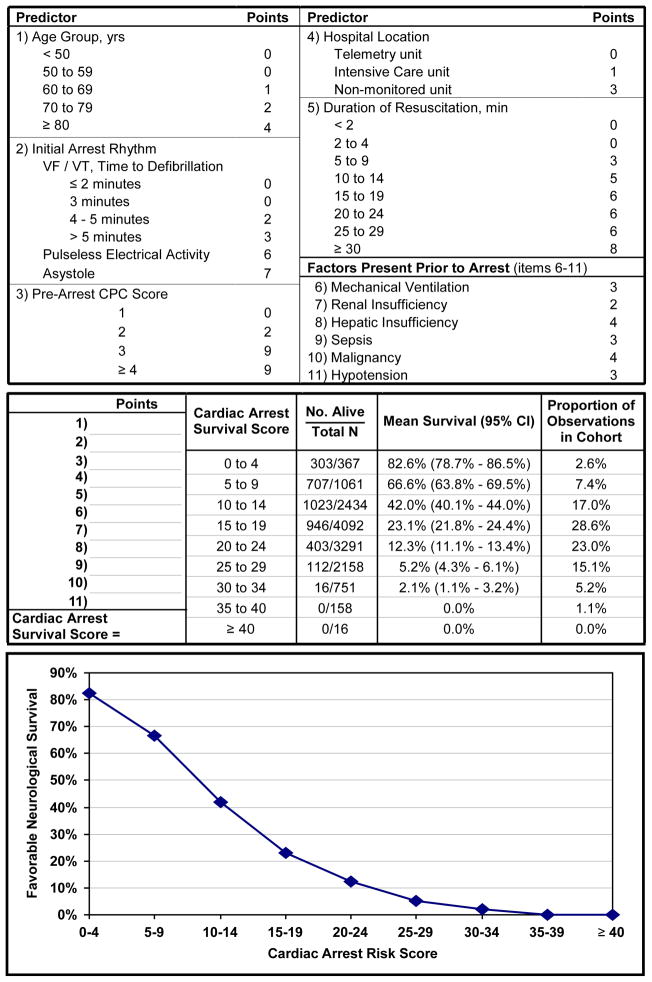
Results: Rates of favorable neurological survival were similar in the derivation cohort (7052 patients [24.6%]) and validation cohort (3510 patients [24.5%]). Eleven variables were associated with favorable neurological survival: younger age, initial cardiac arrest rhythm of ventricular fibrillation or pulseless ventricular tachycardia with a defibrillation time of 2 minutes or less, baseline neurological status without disability, arrest location in a monitored unit, shorter duration of resuscitation, and absence of mechanical ventilation, renal insufficiency, hepatic insufficiency, sepsis, malignant disease, and hypotension prior to the arrest. The model had excellent discrimination (C statistic of 0.80 for both the derivation and validation cohorts) and calibration. The prediction tool demonstrated the ability to identify patients across a wide range of rates of favorable neurological survival: patients in the top decile had a 70.7% probability of this outcome, whereas patients in the bottom decile had a 2.8% probability.
Conclusions: Among successfully resuscitated patients with an in-hospital cardiac arrest, a simple, bedside prediction tool provides robust estimates of the probability of favorable neurological survival. This tool permits accurate prognostication after cardiac arrest for physicians, patients, and families.
Conflict of interest statement
Figures
Comment in
-
Prediction of "mostly dead" vs "all dead" after in-hospital cardiac arrest.Arch Intern Med. 2012 Jun 25;172(12):954. doi: 10.1001/archinternmed.2012.2279. Arch Intern Med. 2012. PMID: 22641335 No abstract available.
References
-
- George AL, Jr, Folk BP, 3rd, Crecelius PL, Campbell WB. Pre-arrest morbidity and other correlates of survival after in-hospital cardiopulmonary arrest. Am J Med. 1989 Jul;87(1):28–34. - PubMed
-
- Cohn EB, Lefevre F, Yarnold PR, Arron MJ, Martin GJ. Predicting survival from inhospital CPR: meta-analysis and validation of a prediction model. J Gen Intern Med. 1993 Jul;8(7):347–353. - PubMed
-
- Cooper S, Janghorbani M, Cooper G. A decade of in-hospital resuscitation: outcomes and prediction of survival? Resuscitation. 2006 Feb;68(2):231–237. - PubMed
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003 Sep;58(3):297–308. - PubMed
-
- Cummins RO, Chamberlain D, Hazinski MF, et al. Recommended guidelines for reviewing, reporting, and conducting research on in-hospital resuscitation: the inhospital ‘Utstein style’. American Heart Association. Circulation. 1997 Apr 15;95(8):2213–2239. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
