

Abnormal initiation and conduction of slow-wave activity in gastroparesis, defined by high-resolution electrical mapping
- PMID: 22643349
- PMCID: PMC3429650
- DOI: 10.1053/j.gastro.2012.05.036
Abnormal initiation and conduction of slow-wave activity in gastroparesis, defined by high-resolution electrical mapping
Abstract
Background & aims: Interstitial cells of Cajal (ICC) generate slow waves. Disrupted ICC networks and gastric dysrhythmias are each associated with gastroparesis. However, there are no data on the initiation and propagation of slow waves in gastroparesis because research tools have lacked spatial resolution. We applied high-resolution electrical mapping to quantify and classify gastroparesis slow-wave abnormalities in spatiotemporal detail.
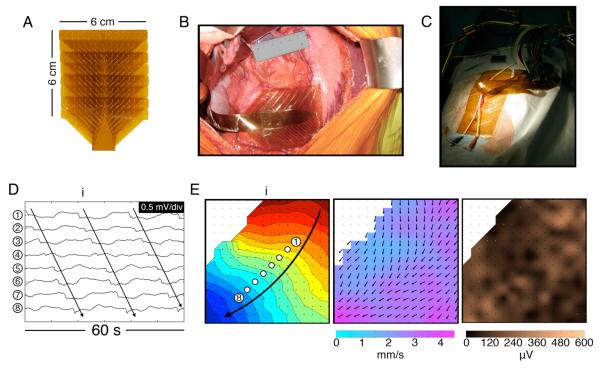
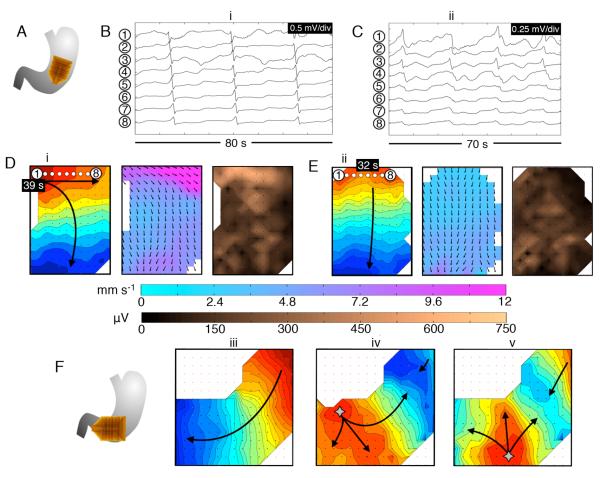
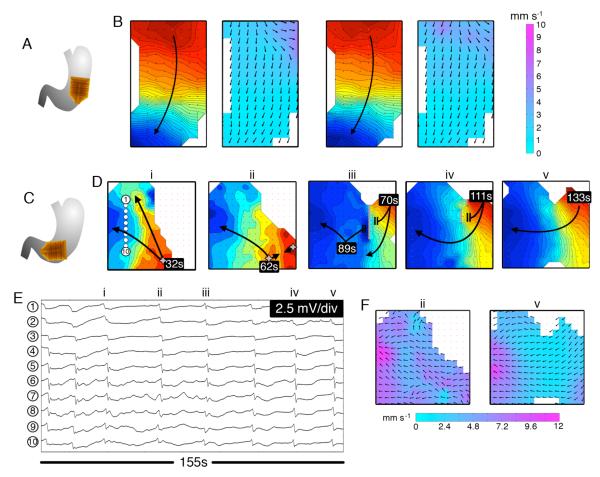
Methods: Serosal high-resolution mapping was performed using flexible arrays (256 electrodes; 36 cm(2)) at stimulator implantation in 12 patients with diabetic or idiopathic gastroparesis. Data were analyzed by isochronal mapping, velocity and amplitude field mapping, and propagation animation. ICC numbers were determined from gastric biopsy specimens.
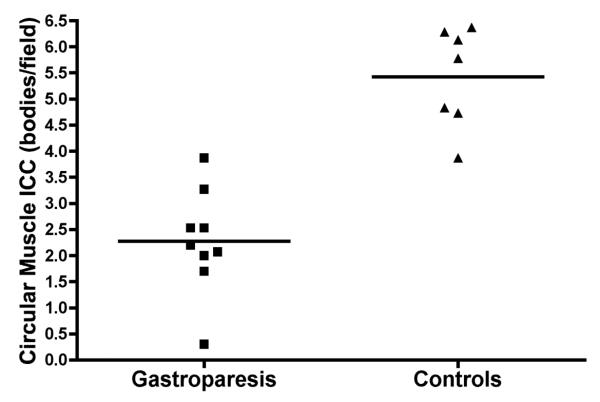
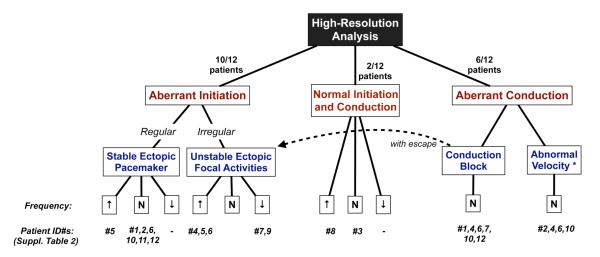
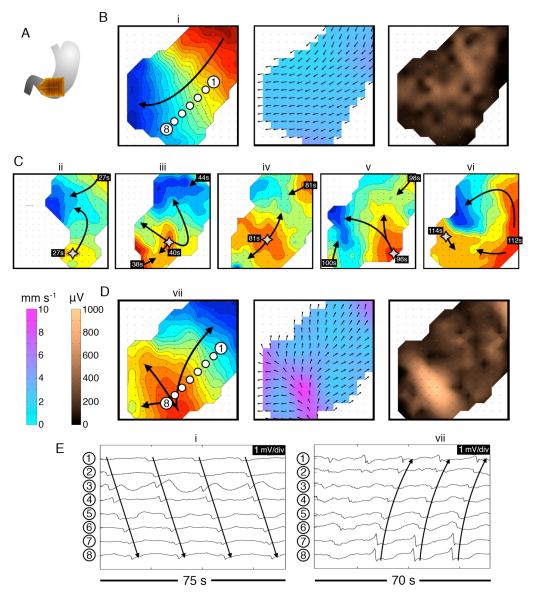
Results: Mean ICC counts were reduced in patients with gastroparesis (2.3 vs 5.4 bodies/field; P < .001). Slow-wave abnormalities were detected by high-resolution mapping in 11 of 12 patients. Several new patterns were observed and classified as abnormal initiation (10/12; stable ectopic pacemakers or diffuse focal events; median, 3.3 cycles/min; range, 2.1-5.7 cycles/min) or abnormal conduction (7/10; reduced velocities or conduction blocks; median, 2.9 cycles/min; range, 2.1-3.6 cycles/min). Circumferential conduction emerged during aberrant initiation or incomplete block and was associated with velocity elevation (7.3 vs 2.9 mm s(-1); P = .002) and increased amplitudes beyond a low base value (415 vs 170 μV; P = .002).
Conclusions: High-resolution mapping revealed new categories of abnormal human slow-wave activity. Abnormalities of slow-wave initiation and conduction occur in gastroparesis, often at normal frequency, which could be missed by tests that lack spatial resolution. Irregular initiation, aberrant conduction, and low amplitude activity could contribute to the pathogenesis of gastroparesis.
Copyright © 2012 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Motility: Mapping gastric dysrhythmias in gastroparesis--a slow wave of electrical activity.Nat Rev Gastroenterol Hepatol. 2012 Jun 19;9(7):363. doi: 10.1038/nrgastro.2012.116. Nat Rev Gastroenterol Hepatol. 2012. PMID: 22710570 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
